 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
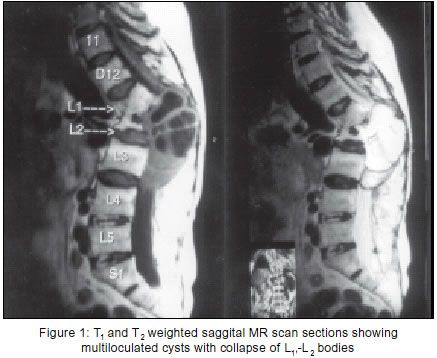
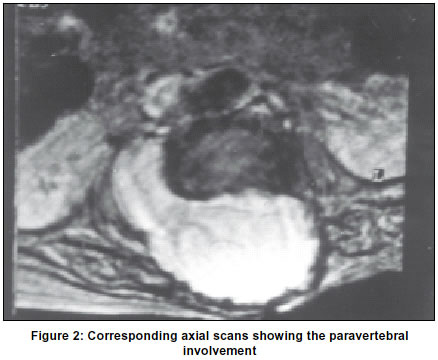
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 89-90 Case Report Primary spinal extradural hydatid cyst N. K. Sharma, N. Chitkara, N. Bakshi, P. Gupta Department of Neurosurgery, Pt. B.D.S. PGIMS, Rohtak, India. Accepted on 06.09.2001. Code Number: ni03025 We report a rare case of spinal cord compression caused by primary multiple extradural hydatid cysts. Key Words: Hydatidosis, spinal hydatid cyst. Hydatid disease occurs in humans as a result of faeco-oral contamination. It affects the bones in 0.5-2% of cases,1,2 of which spine is involved in approximately 45% of cases.1-3 In the vertebral column it affects the lumbar, thoracic and cervical region, in decreasing order of frequency.1 It begins as a single primary cyst which contains daughter cysts. Rupture of such cysts into the muscle is followed by formation of secondary cysts. Here we report one such case along with a review of literature. Case Report A 40-year-old female presented with complaints of gradually increasing, low backache and altered sensations in the perineal and thigh region. Soon, she developed hesitancy of micturition. On examination, there was 50% loss of all forms of sensations bilaterally and symmetrically in the saddle distribution. Motor deficit was not marked where ankle reflex was absent on both sides. MR examination of the lumbosacral spine showed collapse of L1-L2 vertebral bodies and L1-L2 disc space could not be identified (Figure 1). Posteriorly, the region of spinal canal showed multiseptate lesion (hypointense on T1 and hyperintense on T2 weighted images with hyperintense margins). There was involvement of paraspinal muscles in scans (Figure 2). T12 to L3 laminectomy was done and multiple cysts seen in an extrapouch located extradurally on the right side were removed. Cord decompression was done. The operation area was soaked with 3% normal saline-wetted patties for 5 minutes and the area was then washed with normal saline. The diagnosis of hydatid disease was confirmed on histopathology. Early postoperative neurological examination revealed no improvement. The neurological deficit receded in another 2-3 weeks time. Postoperatively, mebendazole was given orally for one year. During the follow-up period of one year, repeated clinical, radiological and serological examinations did not show any evidence of systemic hydatidosis. Discussion Echinococcosis is a widespread disease that appears during the evolution of the parasite echinococcus granulosus. Hydatidosis of the spine was first described by Churrier in 1807.4 In hydatid cyst diseases, vertebral involvement occurs in 0.2-1% of all patients.1-2 Primary vertebral hydatid disease without any other systemic involvement can occur with direct portovertebral venous shunts.5 Whether the thoracic6,7 or the lumbar1 region is more commonly involved is controversial. The cyst can be located epidurally and may be single or multiple. Intradural and extramedullary involvement is rare.8 45% of such patients are under 30 years of age. Generally, spinal hydatid cyst disease present with radicular symptom or symptom of cord compression.9 On plain X-ray, osseous changes are found in 27% of cases and "moth eaten areas" with surrounding sclerosis are typical.10 The operative procedure of choice is laminectomy. However, decompression with anterior vertebrectomy and fusion also gives good results.8 In the series published by Necmettin Pamir M et al,8 neurological improvement was seen in 63% of the cases and recurrence in 18%. Overall, a recurrence rate of 30-40% is described.11 There is a correlation between cyst localization and recurrence. In the epidural osseous type of cysts, there are microvesicles which are spread diffusely inside the bone ("cystic disease of the vertebrae") and these cysts usually rupture during the surgical procedure causing recurrence.11,12 Recurrence is very rare with the intradural extramedullary form of the disease. To prevent recurrence it has been recommended that hypertonic saline solution be used during surgery. Mebendazole has an established lethal effect on secondary E. granulosus cyst, and can be used in the pre-, peri- and post- operative periods.5 However, the overall efficacy of this drug must be evaluated after a more prolonged period of observation. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03025f1.jpg] [ni03025f2.jpg] |
| |||||||||

{kind=link}
{kind=link}