 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
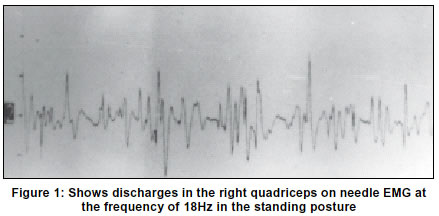
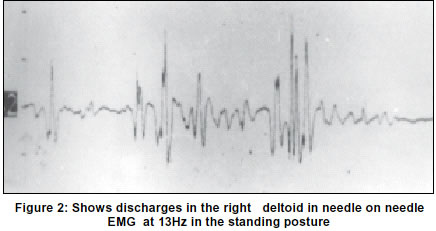
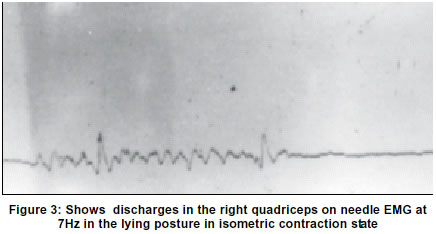
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 91-93 Case Report Orthostatic tremor: report of a case and review of the literature K. B. Bhattacharyya, S. Basu, A. D. Roy, S. Bhattacharya Department of Neurology, Calcutta National Medical College and Hospital, Calcutta, India. Accepted on 13.11.2001. Code Number: ni03026 Orthostatic tremor is a rare movement disorder characterized by tremulousness of the lower limbs on standing that disappears on walking, sitting or on lying down and a distinctive electromyographic burst of 14 to 16 Hz. On inspection, fine ripples can sometimes be seen over the quadriceps on standing. The tremor has a tendency to reappear even in the supine posture if the lower limb muscles are put to an isometric contraction state, indicating thereby that in spite of the fact that the tremor occurs on standing, it is essentially `orthostasis independent' and the central factor is the contraction of the muscles. As a matter of fact, the tremor is abolished if the subject is suspended by harness, thus relieving him of muscle contraction. Doubts are being cast whether it is a variant of essential tremor since a number of families are being reported to be suffering from this disease as well. Positron emission tomography reveals hyperactivity of cerebellum in orthostatic tremor as it shows in essential tremor, therefore lending credence to such a hypothesis. However, lack of response to alcohol, propranolol and primidone in orthostatic tremor stands out as a serious challenge to such a view. Lack of positive family history, synchrony of contracting group of muscles and negative 'reseting' of the tremor by increasing peripheral load-phenomena consistently observed in orthostatic tremor and not in essential tremor, are other features that often help to distinguish between the two conditions. We report a case of orthostatic tremor that presented with the classical clinical and eletromyographic features. Relevant literature in this regard is also being reviewed. Key Words: Orthostatic tremor, Electromyography, Essential tremor. Heilman in 1984 coined the term `Orthostatic Tremor' (OT) to describe quivering movements of the legs and trunk during quiet standing, accompanied by a curious sensation of unsteadiness that was relieved by walking or leaning against objects.1 The condition is characterized by a distinctive 14 to 16 Hz lower extremity bursts in electromyography (EMG), evoked on standing but not while walking or on assuming supine position. There are reports that the tremor makes its appearance in the hands as well, if the subject assumes a crouching posture, with palms and toes touching the floor. OT disappears completely from the lower limbs, if the subject is lifted off the ground.2 The characteristic tremor frequency is also seen in the upper limb muscles during quiet standing in some cases. It may therefore, be considered a disease of station rather than of gait. Judging from the observation that contractions of the muscles, be they in the lower or the upper limbs is central in the genesis of OT, some authors believe that OT is a variant of essential tremor (ET). This is buttressed by the observation that a family history of ET, head tremor or arm tremor often coexists with OT and the burst of tremor has a wide range of frequency (6 to 20Hz).4,5,6 However, lack of response of OT to alcohol, beta blockers and primidone, the absence of family history and the high degree of synchrony between different groups of contracting muscles militate against such a contention. The abnormal bilateral cerebellar hyperactivity, detected by position emission tomography (PET) studies in OT is also akin to changes in ET and primary writing tremor, supports this hypothesis.7,8 The general consensus is that OT is mediated by a central oscillator.9,10 The support for a comes from the observation that external loading does not modify the frequency of the tremor, as it does in enhanced physiological tremor.11 In this respect, it clearly resembles ET. OT usually responds to clonazepam. Other effective agents include primidone, phenobarbiotone, valproic acid and cholorazepate. More recently, gabapentin has also been shown to provide relief for this condition.12 We report a case of OT with classical symptoms and electromyography-revealed burst. Case Report A 70-year-old Muslim male present with complaints of unsteadiness of gait only in the standing position for about a year. He was insistent that he had a premonition of impending fall while standing that vanished within moments of walking or sitting or lying down. He did not complain of such tremulous movement in other parts of the body. There was no antecedent history of mental illness or intake of psychotropic drugs. On examination, we found an individual with perfect mental alertness who had been quivering incessantly in his lower limbs while standing, suggestive almost of an involuntary dance. The movement disappeared when he was asked to walk, sit, lie down or lean against the wall for support. It continued when he was asked to walk backwards and while he was standing unaware of being observed. The quadriceps muscles, while the subject was in the standing posture, showed fine ripples. No such movement was noticed in the upper limbs. There was no tremor in the fingers in the outstretched posture and the rest of the neurological examination was within normal limits. Hemogram, chest X-ray, kidney and liver function tests, electroencephalogram, electrocardiogram and contrast-enhanced CT scan were non-contributory. Concentric needle electromyography of the quadriceps muscles showed discharges of muscle activity at the frequency of 18 Hz (Figure 1), and of the deltoid at 13 Hz (Figure 2). The discharges were not recordable while the subject was supine or had been sitting with the feet dangling. However, they reappeared in the quadriceps when they were put to isometric contraction state in the supine posture and this time the frequency of the discharges was in the range of 7 Hz (Figure 3). Synchronicity of the tremor activity in the corresponding muscles could not be demonstrated for technical reasons. Because of the age of the patient and the low backache that he complained of, we had to abandon the idea of testing muscle burst activity in the crouching posture. The patient was put on clonazepam 0.5 mg per day initially and then gradually increased to 2 mg per day whereupon some improvement was noticed. Increasing the doses further and adding propranolol did not have any beneficial effect. The patient was followed up for a few months and no further improvement or deterioration was observed. Discussion Though Heilman is credited with the distinction of bringing OT to light, it was Pazzaglia et al13 who reported it first. Some authors prefer to call it `primary' in order to indicate its idiopathic nature. OT is a distinctive entity in terms of the clinical and electrophysiological features that distinguish it from other tremulous conditions. The characteristic 16 to 18 Hz EMG bursts in the lower extremities on standing is unique to it and differentiates it from diseases like ET, cerebellar ataxia, myoclonus and clonus due to spasticity where involuntary jerking or leg tremor may be a prominent feature. Some authors however, have described the tremor frequency of OT with a wider range of 6 to 20 Hz.5,6 Importantly, OT is not confined to the lower extremities; it appears in the upper limbs as well if the arm muscles are allowed to contract and it disappears from the lower limbs if they are relaxed, for instance, while the subject is suspended in air by a harness. The tremor disappears on assuming supine posture but makes its appearance if the lower limb muscles are put to isometric contraction state.2 Thus, for many reasons, the condition may essentially be conceived as `orthostasis independent',14 and the mere position of the body, sending afferent signals may not be the crucial factor in the genesis of the tremor. The moot point to answer is the site of origin of the tremor: is it central or peripheral in nature? To a large extent, it can be determined by assessing how the resonance frequency could be modified by changes in external loading of the tremulous limbs. For instance, the mechanical resonance frequency of enhanced physiological tremor, a condition of peripheral origin, is diminished by loading, as reflected in the reduced EMG burst frequency.11,12 This effect however, is not seen in Parkinson's disease or ET, diseases which are mediated by all accounts, by a central oscillator mechanism.12 That the tremor frequency in OT did not change while additional load was assigned to the subject, thus increasing the body weight, could attest a central oscillatory mechanism, operative in this condition.2,9,10 In general, there are as many as three distinct mechanisms for the production of tremor. Firstly, the seat may be in the motor neurons pool that fire to stimulate the muscles. Synchrony of these motor neurons is controlled by higher order neurons, like the spinal interneurons and the rhythmic firing of these motor neurons with the characteristic frequency of 13 to 16 Hz could be the origin of OT. However, needle EMG recordings in patients with OT have also shown a lower frequency of discharge at about 6 to 8 Hz, thus raising pertinent questions concerning the validity of this concept. Secondly, a combination of central and peripheral mechanisms in the genesis of tremor has also been proposed. However, the tremor frequency of 13 to 18 Hz, characteristic of OT, is just above the range which originates in a lower limb reflex loop. Furthermore, the tremor of OT cannot be `reset' by stimulating the peripheral nerves, an observation that goes against the peripheral nature of origin of the tremor.15,16 Thirdly, certain tremors are generated by central oscillation alone. The high degree of synchrony between different groups of contracting muscles OT and the fact that OT may be `reset' by magnetic stimulation of the cortex, the theory of central origin.1,15,17 However, this has been contested by other workers.18 A very recent and important work however, questions whether the complex task-dependent timing relations of rhythmic postural muscle activity are the underlying primary pathology of OT. It was proposed that the peripheral manifestations of muscle bursts merely unmask the normal central processes and may provide a clue to the nature of postural motor control.19 In a recent paper, Sander et al analyzed the electrophysiological correlates of two subjects with OT.20 The study included acclerometric recordings in the legs, the instrument being placed over the vastus medialis muscle just above the knee. The acelerometric frequency was in the same range of 16 to 17 Hz as were the EMG bursts from the lower limb. Mental concentration also failed to `reset' the tremor. Furthermore, one of the two subjects sustained head injury two weeks before the onset of OT. A similar sort of situation has been reported earlier by Sanitate et al, attesting a clinical state that is not associated with ET, thus helping once again to define ET as a different and distinct entity.21 Coexistence of OT and ET has also been reported and either co-inheritance or an undermined genetic defect may underlie this phenomenon.4,6 The association between OT and ET has undergone extensive studies. Involvement of the legs in ET is rare. Findley et al22 observed that 15.7% of 185 patients of ET had leg involvement, while `pure' leg tremor, where the hands are spared, was observed in only 2.2%. The oscillation frequency of OT in the range of 14 to 18 Hz in contrast differs from that of ET, in which it hardly exceeds 10 Hz.2,5,16 An interesting observation advanced by Cleeves et al22 suggests that ET of the legs (and not of the hands) can also respond partially to clonazepam and thus this report suggests that the response to clonazepam should not be considered as the `sine qua non' for the diagnosis of OT. The simultaneous occurrence of OT and ET in the same family further strengthens the belief that the two conditions may somehow, be closely related.1,7 One family has been reported by Wee et al7 in which, some members had 7 to 8 Hz tremor in the hands responsive to propranolol, and some others had leg tremor in the range of 6 to 7 Hz, unresponsive to propranolol while clonazepam reduced the tremor to some extent. This report provides adequate argument in favour of their strong association and Sehrag et al25 have recently described a case of unusual jaw tremor that had the characteristics of OT. Moreover, the observation that in both OT and ET, there is abnormal cerebellar activity, as evidenced by PET study,7,8 or that peripheral loading does not alter the frequency of tremor in any of the situations11,12 suggesting thereby, the operation of a central oscillator9,10 and contend strongly in favour of a close relationship between the two conditions. Papa et al5 from all the evidence advanced from different workers suggested that OT might represent part of the spectrum of ET as do primary writing tremor, isolated head tremor, voice tremor and others and it is possible that the common features of both the varieties of tremors could be initiated by adoption of certain postures that induce muscular contraction. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03026f2.jpg] [ni03026f1.jpg] [ni03026f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}