 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 94-97 Case Report Functional MR imaging of hand motor cortex in a case of persistent mirror movement P. N. Jayakumar, J. M. E. Kovoor, S. G. Srikanth, A. B. Taly,* V. Kamat* Departments of Neuroimaging and Interventional Radiology and *Neurology, National Institute of Mental Health and
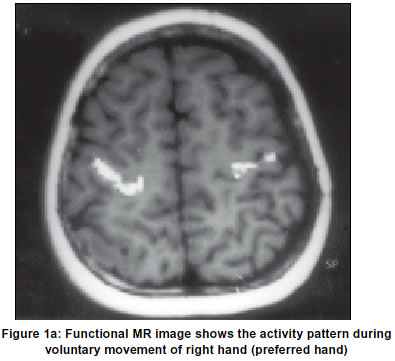
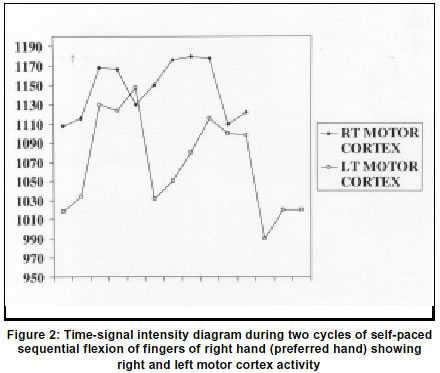
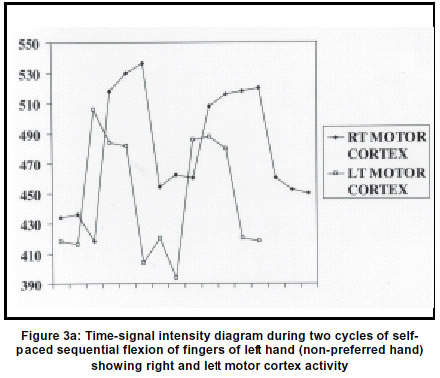
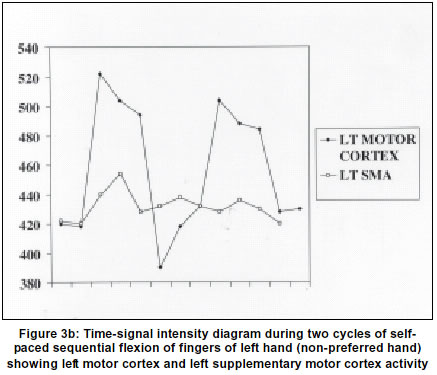
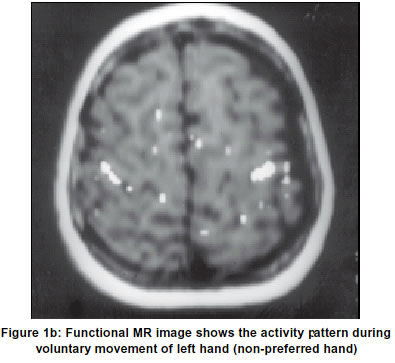
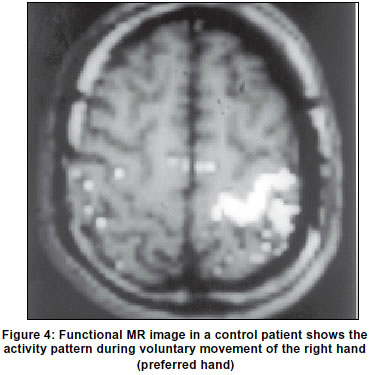
Neurosciences, Bangalore-560029, India. Accepted on 04.12.2001. Code Number: ni03027 Persistent mirror movements are unwanted movements restricted to muscles homologous to those moved intentionally on the opposite body half. It is rarely observed and the functional MRI findings in a case of persistent mirror movement are described. Key Words: Functional MR imaging, MRI, Mirror movements, Brain function. Persistent mirror movements can be defined as associated or synkinetic movements that are executed involuntarily by a muscle group or limb on one side of the body in response to an intentionally performed movement in the corresponding contralateral muscle group or limb.1 They are considered normal in early childhood and may not be clinically demonstrable after eight to ten years of age.2 It is pathologic if it persists or reappears in adults when it is regarded as a sign of delayed maturation or an early damage to the brain.2 It may be seen as an isolated phenomenon without other neurologic findings when inherited as an autosomal dominant trait.1 Neurologic syndromes associated with persisting mirror movements are X-chromosome linked Kallmann syndrome, Klippel-Feil syndrome, phenyl ketonuria, agenesis of the corpus callosum, Usher syndrome, various abnormalities of the spinal cord and diabetes insipidus.1 Surface electroencephalographic and metabolic studies of the cortical activity pattern during unimanual intentional movements in patients with persistent mirror movements show abnormal ipsilateral cortical activity.3,4 The exact pathophysiology of this syndrome is still unclear. Case Report An 8-year-old right-handed girl presented with a history of movement of both hands when only one hand was moved intentionally since the age of three years. No similar family history was present. Clinical examination revealed mirror movements most pronounced in the distal upper extremity and were present in both directions i.e. whenever the right hand was moved the movement was mirrored in the left hand and vice versa. MR imaging was performed on a 1.5T (Siemens Magnetom Vision, Erlangen, Germany) using circular polarized head coil. For anatomic localization, we used a T1W three-dimensional FLASH MR sequence in axial orientation (350/15/90 degrees-TR/TE/ flip angle, section thickness - 4 mm, FOV210, matrix 128x128). All axial sections were oriented parallel to the ac-pc (anterior commissure-posterior commissure) line. After obtaining the anatomic MR images, 100 functional measurements were obtained using 10 sections in the axial plane. Multishot EPI sequence using BOLD contrast was used (1.68/64/1650/90 degrees-TR/TE/TD/flip angle with section thickness of 4 mm, FOV210, matrix 128x128). It covered all of the primary hand motor cortex and the cingulate gyrus. During measurement, a rest-activation paradigm was used with 10 measurements each, a total of 5 sets. During the activation period, the patient performed rapid self-paced sequential flexion of all the fingers of the right hand at approximately 1Hz. The same procedure was repeated with the left hand. The active and rest measurements were grouped separately. Activity curves were grouped for each slice and a suitable z-score thresholding was done. The resulting z-score images of individual slices were grouped to obtain Time-Activity curve (TAC). The z-score image of each slice was superimposed on the T1WI. The images of each slice were compared for activity for the preferred (Figure 1a) and non-preferred (Figure 1a) hand movements. The time-activity curves between the ipsilateral (Figure 2) and contralateral activity (Figures 3a & b) were compared to identify the latency between the two sides. Time signal intensity diagrams were obtained at the region of interest over the precentral gyrus to evaluate the signal intensity change in the primary motor area using auto display and Z-scoring. Areas with marked signal intensity were superimposed on the corresponding anatomic MR image allowing exact spatial localization of functional information with anatomical structure. In our case functional MR imaging showed activity at the following sites (a) the central sulcus medially at the superior bend bilaterally, with more area on the contralateral side, (b) lateral part of the central sulcus bilaterally, (c) in the post central sulci of both hemispheres, (d) in the medial region of the contralateral precentral sulcus (e) rostral to the precentral sulcus in a paramedial location. Time-activity plots show similar excursions of both motor cortex intensity plots during separate voluntary activation of the preferred and non-preferred hands and activation of the left SMA (supplementary motor area) with left hand activity. There was latency in the activation of the right motor cortex compared to left motor cortex with non-preferred hand activity (Figure 3a). Control studies in six healthy volunteers (Figure 4), in the age group of 30 to 45 years showed activity only in the contralateral motor cortex. Discussion Comparison with the control studies in six healthy volunteers showed activity only in the contralateral motor cortex. No activity was seen in the ipsilateral side. Ipsilateral activity has been demonstrated in normal controls in a few of the studies, best in fMRI and PET studies.5-7 Complex studies have documented activity in addition, in the premotor cortex, sensory cortex and the supplementary motor area. The finding of bilateral activity in our patient is similar to the report of a larger study.5 Such findings have also been documented with SPECT/PET and electrophysiological studies.3,4,8,9 An interesting observation in our patient was the significantly increased activity on the ipsilateral side with both the preferred and non-preferred hand motions. While some studies have shown proximal ipsilateral activity with the non-preferred hand,10-12 proximal ipsilateral activity was seen with both the hands in our patient. The TA (time-activity) curves in our patient suggest simultaneous onset of activity in both the motor cortices. This would confirm the findings of Leinsinger et al5 and their unifying theory of corticospinal fibre decussation and bilateral cortical activation. Our finding of higher ipsilateral activity as compared to control would suggest proximal ipsilateral innervations contrary to normal. This has been demonstrated by measurement of cortical potential by Mayer et al.3 They observed prominent ipsilateral activity, which suggested a large uncrossed motor pathway with supplementary recruitment from the ipsilateral side during initiation of movement. Although the exact pathophysiology of persistent mirror movements is unknown, various hypotheses are propounded. Some authors hypothesize that single motor cortical neurons bifurcate and establish a connection on both sides of the spinal cord.13 Leinsinger et al5 propose a unifying model based on two plausible assumptions: (a) a voluntary movement of certain strength requires a corresponding degree of afferent synaptic activity to excite spinal cord motor neurons, and (b) the space available for such synapse does not differ in patients with mirror movements as compared with that in healthy subjects. In such a patient with bifurcating corticospinal axons, the normal activity of corticomotor neurons in the hemisphere contralateral to the movement may not be sufficient to overcome the spinal threshold for excitation. Additional synaptic activity would only be provided by axons originating in the hemisphere ipsilateral to the moving limb. The activity in the superior bend of the central sulcus has been validated as the hand representation in the primary motor cortex by correlating intraoperative cortical stimulation with functional MR imaging findings.7 Activity found in the precentral, post-central, and paramedial regions, possibly representative of the activity of the premotor area, primary sensory cortex, and the supplementary motor area respectively, has been ascribed to the complexity of the motor task used during measurement.6 In the study by Leinsinger et al,5 five patients with persistent mirror movements were compared with ten healthy control subjects using a two-dimensional FLASH functional MR sequence with blood oxygen level dependent (BOLD) contrast. Their study during unimanual intentional movements in control population showed activity in the superior bend of the central sulcus along the characteristic knob of the pre-central gyrus contralaterally, lateral part of the central sulcus ipsilaterally, medial region of the pre-central gyrus, pre-central and post-central gyrus of both hemispheres and rostral to the precentral sulcus in a paramedial location that probably corresponded to the supplementary motor area. In their patients, population areas of increased signal intensity were seen on the contralateral side comparable to the control. All patients differed from the control subjects in the additional presence of activity in the superior bend of the ipsilateral central sulcus, which was of smaller size compared with the activated area during intentional movement of the opposite hand. Our case also showed similar finding of activity in the superior bend of the central sulcus bilaterally on unilateral intentional movement. Time-activity plots show similar excursions of both motor cortex intensity plots during separate voluntary activation of the preferred and non-preferred hands and activation of the left SMA with left hand activity. There was latency in the activation of the right motor cortex compared to left motor cortex with non-preferred hand activity. This indicates that (a) there is bilateral motor cortex activation with voluntary movement of either preferred or non-preferred hand with greater recruitment of the ipsilateral motor cortex due to greater amount of uncrossed fibers, (b) there is latency in activation of the right motor cortex with the non-preferred hand voluntary movement and (c) non-preferred hand voluntary activity is reinforced by recruitment of left SMA due to greater amount of uncrossed fibers. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03027f3a.jpg] [ni03027f3b.jpg] [ni03027f1b.jpg] [ni03027f4.jpg] [ni03027f2.jpg] [ni03027f1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}