 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
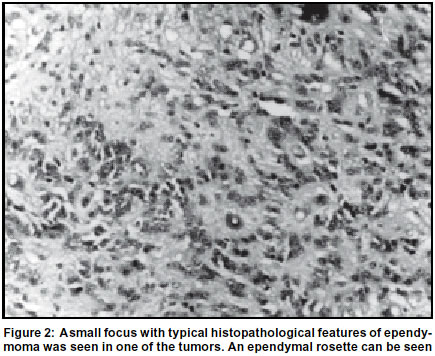
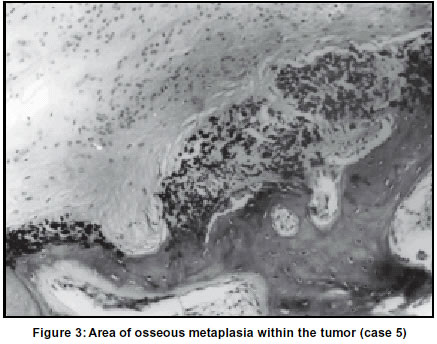
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 98-99 Case Report Subependymomas in children: A report of five cases including two with osseous metaplasia M. K. Mallik, N. Babu, N. Kakkar, V. K. Khosla,* A. K. Banerjee, R. K. Vasishta Department of Histopathology and *Neurosurgery, Postgraduate Institute of Medical Education and Research, Chandigarh-160012, India. Accepted on 07.12.2001. Code Number: ni03028 Subependymomas are highly differentiated slow growing gliomas. They are one of the few gliomas which are biologically benign. They are extremely rare in children. However, after going through the histopathology records of our department of fourteen years (1983-1997) we found that five (20%) cases of subependymomas have been diagnosed in children out of a total of twenty-six subependymomas. Two of our cases showed the presence of osseous metaplasia, a hitherto undescribed finding. Key Words: Subependymoma, Children, Osseous metaplasia. Subependymomas are highly differentiated slow growing gliomas composed of ependymal and astrocyte-like cells. These occur in the walls of the ventricular system or rarely in the parenchyma of the spinal cord.1 They are one of the few gliomas which are considered biologically benign. Most often, they are encountered as incidental post-mortem findings and only occasional examples are seen as surgical specimens.2 Children are rarely affected.1 In this article, we describe five cases of subependymomas in children who presented with neurological symptoms. The age ranged from four-and-a-half to six years. In addition, bony metaplasia, hitherto undescribed in these tumors, was seen in two cases. Case Report After reviewing the histopathology records of the Department of Histopathology, PGIMER, Chandigarh, we found five cases of subependymomas reported over a period of fourteen years (1983-1997) among pediatric patients. Altogether twenty-six subependymomas were diagnosed during this period. The hematoxylin and eosin stained slides were reviewed and the clinical and radiological details were obtained from the hospital records. For the histopathological diagnosis, strict criteria were used and tumors where areas of both subependymoma and ependymoma were present were diagnosed as subependymomas only when the overwhelming majority of the area was subependymomatous. In three of our cases immunostaining for glial fibrillary acid protein was performed. All the five patients were males (age range 41/2-6 years) who presented with features of raised intracranial tension for three to six months. One of them had a history of diminished vision for three months and frequent falls for five months. In two cases, there was a recurrence within one year of surgery. In one case the child expired due to postoperative complications within one week of surgery. In the remaining two cases there was no recurrence. The salient findings have been summarized in Table 1. In all these cases, the tumors were received as greyish white firm fragments. In two of these cases gritty hard areas were felt on slicing. Microscopically typical histology of subependymoma was seen. A sweeping of highly fibrillar processes about clustered nuclei was noted. The nuclei were oval shaped with homogenous pale chromatin and minimal pleomorphism (Figure 1). The interface between the tumor and the brain was sharp. In one of our cases, small foci within the tumor showed features of ependymoma (Figure 2). However, because this accounted for a very small proportion of the tumor area (approx. 5%), the tumor was labeled as subependymoma. The histology did not give any indication of a higher grade in the recurrent cases. In two cases prominent osseous metaplasia associated with areas of calcification were seen (Figure 3). In both these lesions radiological examination had detected this change. These areas of osseous metaplasia were intimately admixed with the tumor area. Immunostaining for glial fibrillary acid protein was positive in the tumor area but not in the area of bony metaplasia. Discussion Subependymomas are one of the few gliomas which are considered biologically benign.1 They usually occur in adults.1 Only one case report is available in the literature describing a subependymoma in a two-and-a-half year old boy.3-5 Out of twenty-six cases of subependymomas diagnosed in our department within a period of fourteen years, five belonged to the pediatric population (approx. 20%). Our hospital series mainly consisted of the North Indian population. Whether this higher incidence is due to a geographical variation is a matter of debate. One child expired within one week of surgery due to postoperative complications. Out of the remaining four, two cases recurred and two did not show any recurrences. The recurrences were successfully treated and the patients are doing well till date. Two of the five cases showed osseous metaplasia. Various CNS tumors are known to show metaplastic elements like epithelial tissue, bone, cartilage and skeletal muscle.6-8 Astrocytomas, glioblastomas, ependymomas and medulloblastomas6-8 are some such tumors which show the presence of metaplastic elements. The most possible mechanism for the formation of such elements is the metaplasia of the supporting connective tissue.6-8 In addition, neoplastic glial cells may also secrete substances which can lead to the formation of these elements.8 There are reports of sarcomatous proliferation in the vasculature of subependymomas9 and a report of rhabdomyosarcomatous differentiation.10 However, we have not come across any report of osseous metaplasia in subependymomas. Thus the finding of bony metaplasia in two of our five cases is unusual as calcification and ossification was observed on X-Ray/CT. Since one of the most common posterior fossa SOL in children, the medulloblastoma, rarely ossifies, tumors in children with calcification and ossification as indicated by radiological examination may suggest subependymomas. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03028f3.jpg] [ni03028f1.jpg] [ni03028t1.jpg] [ni03028f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}