 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 100-101 Case Report Ocular myasthenia gravis coincident with thyroid ophthalmopathy A. Yaman, H. Yaman* Isparta State Hospital, Dept. of Neurology, Isparta, Turkey, and
*Akdeniz University, Medical School, Dept. of Family Medicine, Antalya, Turkey.
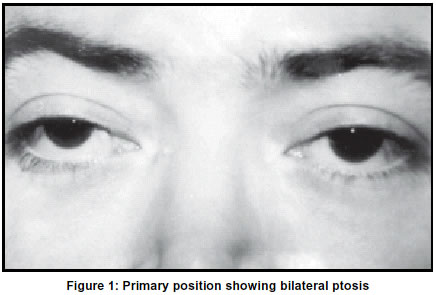
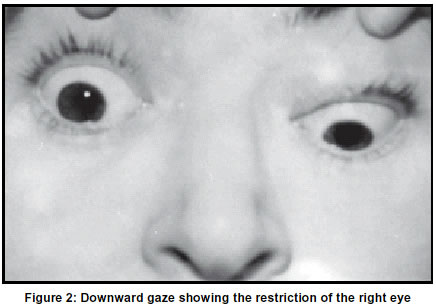
Accepted on 01.02.2002. Code Number: ni03029 Graves' disease and myasthenia gravis are both auto-immune diseases and the coexistence of these two diseases is well recognized. Myasthenia gravis is more frequent in patients with thyroid disease. Here we present a case of thyroid ophthalmopathy and ocular myasthenia. Key Words: Myasthenia gravis, Graves disease, Ophthalmopathy, Thymectomy. A 30-year-old woman was admitted with complaints of weight loss, sweating, palpitation and tremulousness for about 4 months. The patient was diagnosed to have Graves' disease. She had a diffuse enlargement of the thyroid gland. The routine laboratory investigations including blood glucose level, erythrocyte sedimentation rate, electrolytes, kidney and liver function tests were normal. Complete hemogram showed only a mild iron deficiency anemia. Thyroid function tests revealed free T3: 10,19 pmol/L (Normal values: 3.5-6.5), free T4: 31.84 pmol/L (Normal values :11.5-23.2), TSH: 0,01 mIU/ml (Normal values: 0.35-5.5). Investigation of thyroid antibodies revealed Anti-M: 1020 IU/ml (Normal values: 0-50), Anti-Tg: 17,7 IU /ml (Normal values: 3-50), Tr Ab: 49 IU/ml (Normal values: 0-15). Magnetic resonance imaging (MRI) of the globes showed increased intensity and thickening of both lateral recti, right medial rectus, right superior rectus and left inferior rectus muscles, indicating the infiltration of these muscles, which was consistent with thyroid ophthalmopathy. Propylthiouracil 300 mg/day was started. After two months of propylthiouracil treatment, the patient became euthyroid. Two months after the diagnosis of thyroid disease she developed diplopia on downward and lateral gaze. Three weeks later, bilateral ptosis occurred. The severity of her ptosis fluctuated during the day time. She was examined three days after the onset of ptosis (Figure 1). In physical examination, she had a diffusely palpable thyroid gland and bilateral exophthalmos. The neurological examination revealed bilateral ptosis more on the right side. Diplopia occured during horizontal and downward gaze. Movement of the right globe was restricted during downward gaze (Figure 2). The severity of ptosis increased after sustained upward gaze. Ptosis showed significant improvement after the intramuscular injection of 1.5 mg neostigmine methylsulphate, but the restriction of eye movements did not change. Repetitive stimulation of the right ulnar nerve-adductor digiti minimi muscle and facial nerve-nasalis muscle revealed no decremental response. Acetylcholine receptor antibody level was found to be 1.30 nmol/L, which was more than double the normal levels (normal values:0-0.50). Computed tomography of the thorax revealed a mass lesion of 6 x 3 x 2 cm located in the area of thymus. Pyridostigmine 60 mg four times daily was added for the treatment of ptosis. Exophthalmos and ophtalmoplegia were not relieved but ptosis responded to the treatment. After two sessions of plasmapheresis, the patient was operated. Total thyroidectomy and extended thymectomy were done. Pathological examination showed thymic hyperplasia. After the operation, she was continued on pyridostigmine 60 mg four times daily and levothyroxine sodium 0.15 mg daily. With this treatment, her ophthalmoparesis continued, but ptosis was fairly controlled. Discussion Patients with myasthenia gravis (MG) may have coexisting autoimmune thyroid diseases (AITD), which include auto-immune thyroiditis and Graves' disease. Epidemiological studies show that AITD occur in approximately 5-10% of patients with MG, whereas MG is reported in a fairly low frequency (0.2%) of patients with AITD. The clinical presentation of MG associated with AITD is frequently restricted to eye muscles. Generalized MG was found to be more frequent in patients without thyroid disease. Also, thymic abnormalities were less frequent in MG associated with AITD than in MG without AITD. Although this is not true for patients who have thymic hyperplasia, a greater frequency of thyroid antibodies is reported in ocular MG, when compared to generalized MG.2 The reason for the association of AITD with ocular MG is unknown, but several hypotheses can be considered. First, ocular MG and generalized MG might actually represent separate diseases with different spectra of associated conditions. Second, an immunological cross-reactivity against epitopes or auto-antigens shared by the thyroid and the eye muscles might be the basis of this association. A third explanation for the higher frequency of ocular MG in AITD could be that these disorders have a common genetic background.3 In three-quarters of patients with both conditions, thyrotoxic symptoms occur before or concurrently with those of myasthenia.4 Our patient had thyrotoxicosis symptoms seven months before her ptosis developed.10 The ocular changes in Graves' disease may include exophthalmos, periorbital edema, lid lag, chemosis and ophthalmoplegia. The extraocular muscles most commonly involved are the superior and lateral recti.1 In our patient, the downward movement of the right eye was restricted and the patient had diplopia during downward and horizontal gaze. Two-thirds of the patients with both disorders show improvement in myasthenia gravis after treatment of thyroid disease.1 The treatment of hyperthyroidism did not improve the myasthenic symptoms in our patient, since her need for anti-acetylcholinesterase medication did not decrease. Some authors state that thymectomy may have positive effects on both myasthenia5 and AITD.3 Our patient did not show any obvious improvement after thymectomy. In conclusion, we report that the coexistence of MG with AITD might have prognostic relevance and occurs in a subgroup of MG patients with a mild form of the disease. It should be remembered that, ptosis is not an expected symptom in thyroid ophthalmopathy. If ptosis or paresis of the orbicularis oculi muscle develops in a patient with thyroid ophthalmopathy, coincidence of myasthenia gravis should be considered. Acknowledgement This case report was presented as a poster presentation at the 5th EFNS Congress in Copenhagen, Denmark. We thank Dr. C. Isikay and Prof Dr. N. Mutluer for their contributions during the preparation of this case report. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03029f1.jpg] [ni03029f2.jpg] |
| |||||||||

{kind=link}
{kind=link}