 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 110-111 Short Report Cerebral salt wasting syndrome in a patient with a pituitary adenoma S. K. Singh, A. G. Unnikrishnan, V. S. Reddy, R. K. Sahay, S. K. Bhadada, J. K. Agrawal Department of Endocrinology and Metabolism, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221005, India.
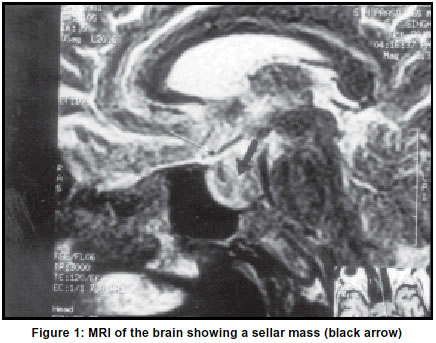
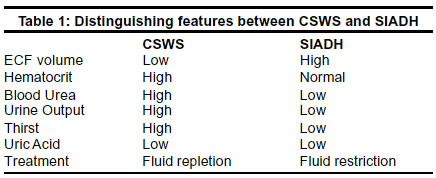
Accepted on 21.03.2001. Code Number: ni03032 Cerebral salt wasting syndrome (CSWS) is often an unrecognized cause of hyponatremia that occurs in the setting of intracranial lesions. It is important to differentiate CSWS from the syndrome of inappropriate ADH secretion, as this would alter the management of hyponatremia. We describe a case of CSWS that occurred in association with a nonfunctioning pituitary adenoma. Key Words: Hyponatremia, Cerebral salt wasting syndrome, SIADH Cerebral salt wasting syndrome (CSWS) is a clinical syndrome, which is characterized by hyponatremia, hypovolemia and natriuresis.l It occurs in the setting of various intracranial disorders.2 We report an unusual case of CSWS occurring in association with a pituitary adenoma. Case Report A 68-year-old male , after returning from a fortnight-long pilgrimage, developed malaise, became incoherent on the next day and lost consciousness on the third day. There was no history of convulsions or other localizing neurological features. CT-scan revealed an intrasellar mass. On clinical examination, he was dehydrated, but other vital parameters were stable. The patient was unconscious, but had no focal neurological deficits. Systemic examination revealed no other abnormality. Hematological investigations were normal. Serum investigation results were as follows: sodium 118 mmol/L, potassium 3.8 mmol/L, chloride 98 mmol/L, blood glucose 75 mg/dl, blood urea 78 mg/dl, creatinine 1.5 mg/dl, T3 0.7 mmol/L (1.1-2.9), T4 3.5 mmol/L (64-154), TSH 0.8 mU/L (0.5-3.5), morning (8 am) cortisol 3.2 ug/dl (5-25), LH 3 IU/L (5-20), FSH 1.2 IU/L (5-20) and prolactin 20 ng/ml (<15). Urinary spot sodium was 48 mmol/L (20-40) in a urine volume of 4.5 liters in 24 hours. Magnetic resonance imaging showed a well-defined sellar mass (Figure 1) without parasellar or suprasellar extension. A diagnosis of CSWS, in association with a pituitary adenoma (causing central hypothyroidism, hypoadrenalism and hypogonadotropic hypogonadism) was made. Features suggestive of CSWS in our patient were hypovolemia with clinical evidence of dehydration and hyponatremia in association with polyuria. Symptomatic CSWS was probably precipitated by heat exposure and poor fluid intake during the pilgrimage trip. The patient showed clinical improvement after treatment with intravenous saline, thyroxine and glucocorticoids. He was asymptomatic at discharge. Discussion Hyponatremia in association with a sellar mass poses a clinical challenge, because both a decrease in ACTH or an increase in anti-diuretic hormone levels (SIADH) can be the etiological factors. As mineralocorticoid secretion is primarily controlled by the renin angiotensin axis, ACTH deficiency, unless very severe and longstanding, is not usually a cause of hyponatremia. SIADH can occur with sellar lesions; in addition, secondary hypothyroidism as well as ACTH deficiency can worsen preexisting hyponatremia by inducing ADH excess.3 CSWS is an often-unrecognized cause of hyponatremia in intracranial disorders. Its presentation is similar to SIADH, as both present with hyponatremia, and a high urinary sodium concentration.4 However, there are subtle differences (Table 1). Classical causes of CSWS include intracranial lesions, especially head injury, tumors and aneurysm surgery.5 CSWS is attributed to the release of natriuretic peptide from the brain, through stimuli that are unknown.5 It is important to distinguish between CSWS and SIADH, as the former is managed with aggressive fluid therapy (usually with normal saline) while the treatment of SIADH aims at reduction of free water (generally by fluid restriction). In fact, if treatment indicated for one condition is instituted for the other; it aggravates the illness. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03032t1.jpg] [ni03032f1.jpg] |
| |||||||||

{kind=link}
{kind=link}