 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 111-113 Short Report Recurrent intramedullary cervical ependymal cyst R. Chhabra, S. Bansal, B. D. Radotra,* S. N. Mathuriya Departments of Neurosurgery and *Histopathology, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
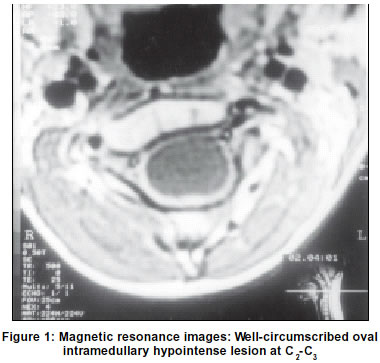
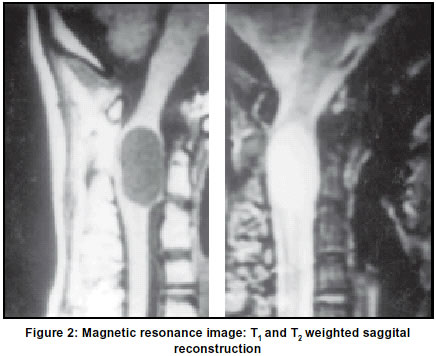
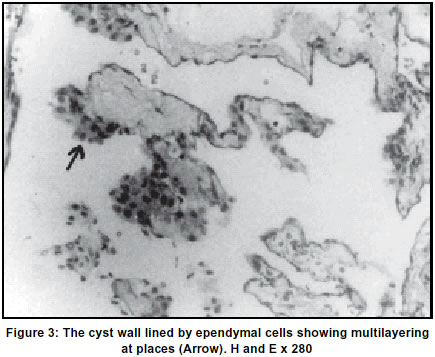
Accepted on 24.03.2001. Code Number: ni03033 We report a rare case of high cervical intramedullary ependymal cyst in a young boy. This was associated with atlantoaxial dislocation. After partial removal and marsupialization, the cyst recurred and needed radical total resection. Key Words: Spinal cord, Cysts, Intramedullary tumors, Ependymal cyst. Spinal intramedullary ependymal cysts are rare. Only eight pathologically proven cases have been reported in the literature.1-11 We report a case of intramedullary cervical ependymal cyst in an adolescent male. Case Report A 15-year-old male presented with complaints of neck pain, restriction of neck movements, quadriparesis and wasting of small muscles of both hands. This followed a trivial fall from a bicycle one month prior to admission. Neurological examination revealed quadriparesis with marked weakness and wasting in distal muscle groups. Both the lower extremities were hypertonic with no sensory impairment. A 4.5 mm fixed atlanto axial dislocation was noted on lateral cervical skiagram. MRI demonstrated a well-circumscribed large oval intramedullary lesion at C2-C3, which was hypointense on T1, and hyperintense on T2 weighted images (Figures l & 2). C2-4 laminectomy was performed. Very thick whitish fluid was drained through a small posterior midline myelotomy. The cyst wall was adherent to the adjacent cord tissue hence a limited excision was carried out and the cyst was marsupialized. Patient regained full function in two months. Histopathology revealed a collapsed cystic structure consisting of a thin fibrous wall lined by flattened to cuboidal ependymal cells showing multilayering at places (Figure 3). After an initial neurological improvement, he worsened again, about a year after surgery, to spastic grade I to III quadriparesis. The involvement was again more marked in the distal muscle groups. MR imaging showed findings similar to the preoperative MRI. At re-exploration, the cyst contents were thick and creamy white. These were evacuated and the wall was cautiously separated off the subjacent cord tissue and resected.The patient showed a steady neurological recovery. Discussion The first patient of intradural ependymal cyst (IDEC) was reported by Hyman et al in 1938.4 Mosso and Verity in 19756 have classified them into intradural extramedullary, intramedullary and mixed variety. The initial two cases of intramedullary ependymal cysts were reported in 1978.3 Subsequently, one case each was reported by Dharker et al2 and Sharma et al.10 Pagni et al8 in 1991 were the first to diagnose a cervical intramedullary ependymal cyst on MRI. Out of the three patients reported by Robertson et al,9 histopathological diagnosis could be established in only one case where the tumor was located in the dorsal cord. Iwahashi (1999) has reported a case of intramedullary ependymal cyst in the dorsal cord in an 18-month-old female.11 These lesions are of developmental origin. The genesis is from extruded ependymal cells located close to the anterior cord substance at the time of closure of the neural tube. These cells are considered to have lost continuity and become isolated from the floor plate of the neural tube.8,15 On histological examination, the lining wall is a single layer of cuboidal cells on fibrous connective tissue. The basement membrane is absent in the cyst wall and contains PAS positive intracytoplasmic glycoprotein. The cases reported by Dharker et al,2 and Wisoff and Ghatak12 possessed basement membrane on histology. The cyst reported by Wisoff and Ghatak12 was found to be endodermal in origin on subsequent review by Hirano et al.15 Recently, Wilkins and Odom14 reported the presence of blepharoplasts in the cystoplasm but this is not a constant finding in all published cases. Electron microscopy can identify the ependymal nature of the epithelium on the basis of intercellular junctions, the characteristics of free surface of the cells, the nucleoplasm and the intracellular inclusions.15 Other ultrastructural and immunocytochemical staining features have recently been described to differentiate ependymal from other cysts.8,9,15 Ependymal cysts are twice commoner in females and occur in the age group of 38 to 71 years.10 These lesions constitute 11% of all the intradural cysts. The distribution is conocaudal in 44%, dorsal in 33% and cervical in 23%. The usual location is anterior to the cord, and hence, the presentation is of motor and spinothalamic deficits.5,8 The onset is usually gradual and the course is progressive, except in the intradural extramedullary cyst reported by Moore,5 which had an acute onset after trauma. Our patient also had a sudden post-traumatic quadriparesis. MRI shows a well-circumscribed cyst with sharp delineation from the cord substance. The contents are of CSF intensity on T1 and T2 weighted images, with no enhancement on Gd DTPA.9,11,16 The location is anterior with a thin layer of cord tissue posteriorly. Our patient also had a fixed AAD (4.5 mm). The cyst wall is inseparable from the cord tissue, except in two cases,8,10 where a plane of cleavage could be established and total excision was possible.8 Earlier, cyst wall biopsy and marsupialization were recommended whenever the the cord tissue was inseparable, as reaccumulation was not reported. The contents were clear in five of the reported cases,11 whereas in our case the cyst had thick whitish contents. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03033f2.jpg] [ni03033f1.jpg] [ni03033f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}