 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
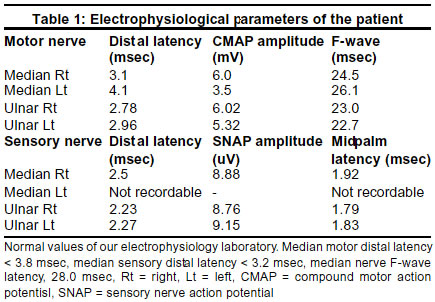
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 113-114 Short Report Carpal tunnel syndrome after 22 years of Colle's fracture V. Goyal, M. Bhatia, M. Behari Department of Neurology, All India Institute of Medical Sciences New Delhi-110029, India. Accepted on 03.04.2001. Code Number: ni03034 Delayed carpal tunnel syndrome is rare. We describe the electrophysiological findings in a patient with Colle's fracture, who developed carpal tunnel syndrome 22 years after a wrist injury. Key Words: Carpal tunnel syndrome, Colle's fracture. Delayed carpal tunnel syndrome (CTS) after Colle's fracture though described as early as 1865 by Sir James Paget,1 is rare. Abboutt and Saunders pointed out the relationship of fracture of lower end of radius and subsequent development of latent median nerve palsy2 but the exact mechanism is not very clear. Cannon and Rochester reported tardy median nerve palsy (TMP) developing 20-50 years after carpal or distal radius and ulnar fractures.1 This complication is higher when there is malunion.3-5 Case History A 65-year-old woman had left Colle's fracture 22 years ago, which was treated conservatively by immobilization. The course was uneventful except for malunion with residual dinner fork deformity. She was asymptomatic till one year ago, when she developed tingling of the left hand in the distribution of median nerve, which was predominantly at night. This gradually increased in severity. On examination, she had no motor or sensory deficit. Median nerve was not palpable. Tinel's sign was positive. She was non-diabetic and euthyroid. There was no other evident cause for CTS. Electrophysiological (EPS) (Table 1) evaluation revealed left median motor latency of 4.1 msec (right-3.1 msec), compound muscle action potential (CMAP) amplitude of 3.5 mV (right- 6.0 mV), and F-wave latency of 26.1 msec (right-24.5 msec). Left median sensory nerve action potential (SNAP) was not recordable (right - distal latency of 2.5 msec, midpalm latency of 1.3 msec and SNAP amplitude of 8.88 µV). The patient was treated with local steroid injection as she refused to undergo surgery for CTS. She had significant relief in her symptoms for 3 months. Discussion CTS is the commonest entrapment neuropathy. Trauma to wrist or Colle's fracture, is known to cause CTS. Acute median nerve compression after Colle's fracture is quite common, and is due to progressive edema and hematoma formation within the carpal tunnel.3,11 Acute CTS is frequently associated with wrist immobilization in a position of marked flexion.12 However, there are few reports of CTS developing after many years following Colle's fracture. In a series of 598 cases with CTS, only 12 (2%) patients had history of wrist injury leading to fracture,9 whereas in another study 11 of the 101 hands operated for CTS had Colle's fracture or carpal bone dislocation.10 The present case developed CTS 22 years after Colle's fracture with malunion. Though CTS can develop after any type of Colle's fracture, it is more common after type 1 (extra-articular) fracture.4 The incidence of CTS after Colle's fracture varies from 0.2-7.9%.6,7,3 The exact mechanism which precipitated CTS 22 years after the injury, is not very clear. As wear-tear and repair are ongoing processes at every joint and synovial cavity, any insult like trauma or fracture can lead to early degenerative changes, which are associated with fibrosis and synovitis. When these changes reach a critical level, it may lead to compression, ischemia of the nerve and pain. The other cause of narrowing of the cross-sectional area of the carpal tunnel, may be a dorsal sublaxation of carpal bones caused by malunited fracture of distal radius.8 Cooney et al found that volar fracture fragments, excessive callous formation and localized swelling were responsible for most cases with CTS.6 References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03034t1.jpg] |
| |||||||||

{kind=link}