 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 117-118 Short Report Phenylpropanolamine-induced intraventricular hemorrhage A. Prasad, K. K. Bhoi, K. Bala, K. S. Anand, H. K. Pal Department of Neurology, Institute of Human Behaviour and Allied Sciences, RML Hospital, New Delhi-110095, India.
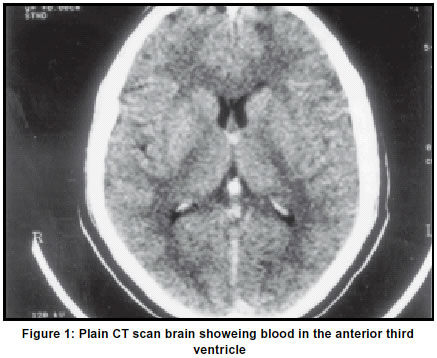
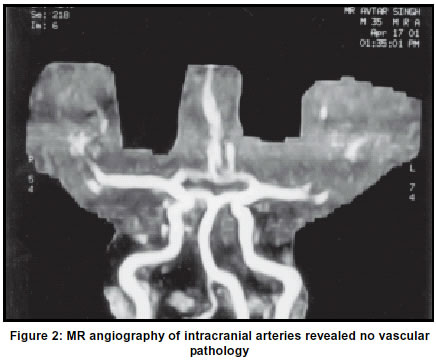
Accepted on 02.08.2001. Code Number: ni03037 Intracranial hemorrhage is an uncommon complication of phenylpropanolamine. There is an increasing awareness of this complication in the West. However, to the best of our knowledge there have been no cases reported from India. Here we report a patient who developed Intraventricular hemorrhage following ingestion of Phenylpropanolamine, from which he made an uneventul recovery over the next two weeks. Key Words: Phenylpropanolamine, Intracranial hemorrhage Phenylpropanolarmine (PPA) is commonly found in over-the-counter (OTC) cough or cold remedies and appetite suppressants. Case reports have linked the use of these products to hemorrhagic stroke, often after the first use.1 Food and Drug Administration (FDA) US, warns of stroke risk associated with PPA, cold remedies and these drugs were removed from store shelves.2 Hemorrhagic stroke following PPA, has not been reported in India so far. A 3-year-old male who developed Intra third ventricular hemorrhage following a tablet of cold remedy containing PPA is reported. Intracranial complications of PPA and causes of hemorrhagic stroke and their outcome are discussed briefly. Case History A 35-year-old male, non-diabetic, non-hypertensive was admitted to neurology ICU with severe headache, vomiting, giddiness, restlessness and slurred speech of one day duration following a tablet of cold remedy (containing PPA-25 mg). There were no associated seizures, loss of consciousness, facial asymmetry, dysphagia or weakness of limbs. He was a non-smoker, non-alcoholic, and not an intravenous drug abuser (IVDA). There was no history of transient ischemic attack (TIA), rheumatic heart disease (RHD), bleeding diathesis or head trauma. On examination, pulse rate was 82/min, regular, all peripheral pulses were normal, no carotid bruit, BP was 130/85 and 140/90 mm Hg in right upper and right lower limb respectively. He was conscious, oriented but restless with normal pupils and fundi and had mild dysarthria. He had horizontal nystagmus grade 1, no motor weakness, normal reflexes, flexor plantar response, mildly ataxic gait and with no signs of meningeal irritation. The rest of the systemic examination was unremarkable. Routine investigations showed a hemoglobin of 13.1 gm/dl, TLC -7520/cmm, DL.C=N80 L17 M01 E02, Hct- 45%, ESR-29mm/ 1st Hr with normal platelet count and coagulation profile, normal routine urine analysis, normal level of blood urea, blood sugar, serum creatinine, and serum Na+, K+. His LFT, lipid profile, ECG, and chest X-ray were normal. Rheumatoid factor, VDRL, ASO titre, and LE cell were negative. A plain CT scan of the head (Figure 1) done on the same day showed blood in the anterior third ventricle. There was no evidence of parenchymal bleeding or hydrocephalus. Lumbar puncture done 48 hrs after the ictus revealed uniformly blood-stained CSF with crenated RBCs and supernatant xanthochromia. On the 2nd day, he developed hesitancy and urinary retention which required catheterization. He was treated conservatively and made a gradual recovery of bladder function by the 6th day. At discharge, he had no nystagmus, dysarthria or ataxia. MRI done on 11th day showed complete resolution of the hemorrhage. MR angiography (Figure 2) of intracranial arteries revealed no vascular pathology. Four vessel angiogram was normal. Two weeks later he had returned to work. Discussion PPA-associated hemorrhagic stroke occurs in young patients (median age - in the early 30 years) usually without a past history of hypertension but with accelerated hypertension in one-third cases on admission. Most hemorrhages occur within minutes to a few hours of ingestion of the drug, usually taken in recommended doses. A survey conducted in the United States between 1994 and 1999 showed that women who use PPA as an appetite suppressant, have a higher incidence of hemorrhagic stroke.4 lntracerebral hemorrhage (ICH) was reported for the first time in a woman of arterio-venous malformation (AVM) after taking diet control pills containing PPA.5 Since then, PPA- associated hemorrhagic stroke has been reported in more than 20 cases.3 Two cases of ICH and one case of subarachnoid hemorrhage (SAH) were reported by Taipa.6 Subsequently, various authors have documented this complication.1,5 Our patient developed Intracranial hemorrhage ten hours after ingestion, for the first time, of low dose PPA (25mg). The pathogenesis of Intracranial hemorrhage due to PPA is unclear. Three women aged 33, 63 and 43 years receiving anorexiant containing PPA, 30 min to 3 hr after medication, presented with frontal hematoma, left putaminal hematoma and SAH respectively.6 Cerebral angiography performed in all of them, did not show any vascular abnormality. It was postulated that the hemorrhage could be related to accelerated hypertension and vasculitis. Beading of Intracranial arteries is frequent in angiogram. It may result from enhanced sympathetic activity, direct vascular effect of PPA, multifocal segmental spasm or less commonly a true vasculitis with transient hypertension in individuals particularly susceptible to the sympathomirnetics.3 Our patient had an Intraventricular bleed documented by non-enhanced CT scan of head and CSF analysis. His angiogram was normal, it did not show any vasculitis, spasm or AVM. The patient developed retention of urine probably related to PPA. Sympathomimetics relax detrusor muscle due to activation of â- receptor and contract trigone and sphincter due to a-agonist activity. It results in hesitancy and retention of urine. PPA also increases urethral pressure.7 PPA is an independent risk factor for hemorrhagic stroke in women.1 Its use should be contraindicated in patients who have family history of vascular anomalies,5 cerebral hemorrhage,4 benign hypertrophy of prostate,8 hypertension and heart diseases. The Committee on Safety of Medicines (CSM) has considered new evidence from the Hemorrhagic Stroke Project. During its meet on 8th Nov 2000, it concluded that PPA is linked to hemorrhagic stroke. CSM has recommended the manufacturers to improve existing product information with prominent warning.4 Steps have been taken by FDA to remove PPA-containing cold remedies and diet control pills from OTC shelves.4 Public education and statutory regulation must be implemented in our country. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03037f2.jpg] [ni03037f1.jpg] |
| |||||||||

{kind=link}
{kind=link}