 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 121-123 Short Report Intracranial aneurysmal bone cyst manifesting as a cerebellar mass S. Kumar, T. M. Retnam, T. Krishnamoorthy,* S. Parameswaran, S. Nair, R. N. Bhattacharya, V. V. Radhakrishanan** Departments of Neurosurgery, *Neuroradiology and **Neuropathology , Sree Chitra Tirunal Institute for Medical Sciences and
Technology, Thiruvananthapurum-695011, India.
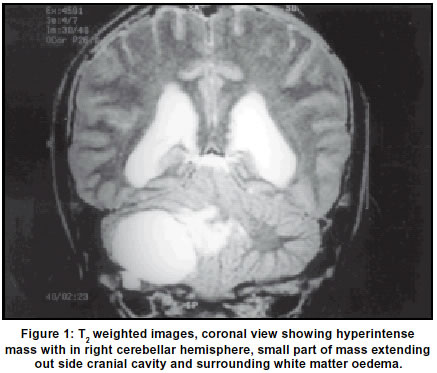
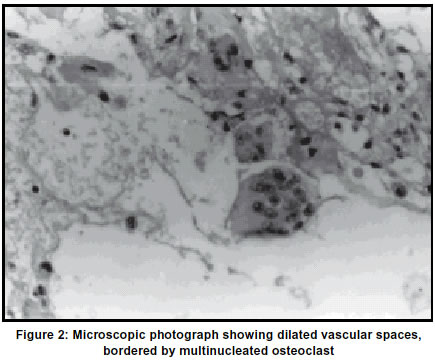
Accepted on 06.09.2001. Code Number: ni03040 A 17-year-old boy presented with symptoms of raised intracranial pressure for a month. Investigations revealed a large extra-cerebellar mass. The lesion was radically resected. It arose from the petrous bone. Histology revealed that the lesion was an aneurysmal bone cyst [ABC]. Key Words: Aneurysmal bone cyst, Benign skull lesion, Intracranial lesion. Aneurysmal bone cyst (ABC) is a benign bony lesion, first described by Jaffe and Lichtenstein in 1942. Most common anatomical location for its occurence of ABC is in the metaphyseal end of long bones and rarely occurs in the skull.1-4 Most cases of ABC manifest before the age of 20 years.3,4 They usually present as palpable skull masses. It is uncommon for calvarial ABC to manifest initially as an intracranial space-occupying lesion. A literature survey revealed 61 cases of ABC.5 We report a case of ABC occurring in the occipital region. Case Report A 17-year-old boy presented with history of headache of one month duration, which was occasionally relieved by bouts of vomiting. He also had dizziness for 2 weeks. Neurological examination revealed bilateral papilloedema. There was no palpable bony lesion over the calvarium. Systemic examination and examination of long bones were normal. Hemoglobin was 16 gm%. CT brain showed a circumscribed right cerebellar, mildly enhancing mass lesion with multiple internal loculations and fluid levels. The lesion caused mass effect on the fourth ventricle and there was a moderate hydrocephalus. MRI scan showed multiloculated isointense lesion on T1W1 with areas of hyperintensity and predominantly hyperintense lesion on T2W1.The mass caused edema in the right cerebellar hemisphere. There was contrast enhancement of septations and the walls (Figure 1). Angiography did not reveal any vascular lesion in the posterior fossa. The patient was taken up for surgery and a midline sub-occipital craniectomy was performed. A large, well-encapsulated, highly vascular tumor arising from the posterior- inferior petrous, posterior to the internal auditory meatus and jugular foramen was identified. There was a defect in the dura and bone at the site of attachment of the tumor. There was a good plane between the lesion and the cerebellum. The lesion had multiple loculi containing blood in different stages of degeneration. The lesion was completely resected. Hematoxylin and eosin-stained sections showed numerous dilated blood spaces and they were devoid of endothelial cells. The vascular spaces were separated by collagenous and osteoid trabeculae, bordered by numerous multinucleated giant cells (osteoclast) (Figure 2). These histopathological findings were consistent with ABC. The patient made an uneventful recovery. Discussion ABC is a benign non-neoplastic lesion of bone, commonly seen in the younger age group, usually before the age of twenty years.2-4,6 Reviewing sixty-one cases, Sheikh et al5 observed that the majority of ABCs occurred in the temporal and occipital bones. The exact pathogenesis of ABC is not well known. Development of focal hemodynamic alterations with secondary venous hypertension was proposed by Lichtenstein.2 Local trauma has also been incriminated in the development of ABC.1,7,8 Bony lesions such as fibrous dysplasia, chondroblastoma, osteoclastoma, non-ossifying fibroma, giant cell tumor, fibromyxoma and unicameral bone cyst were demonstrated to be associated with ABC.4,9,10 Several therapeutic modalities are used for the treatment of ABC, including complete surgical excision or curettage, radiotherapy, cryosurgery and endovascular embolization.2,4,12,13 The treatment of choice for these lesions is total excision, as it is curative.14,15 These lesions being non-neoplastic, the use of radiotherapy is not recommended although it is mentioned in literature.2,3,14 For the same reason, chemotherapy has no role. Endovascular embolization plays an important role in preoperative devascularization of the lesion to reduce intraoperative bleeding. Endovascular embolization can be used in cases where the tumor is located in an area difficult for surgical resection.12,16 References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03040f1.jpg] [ni03040f2.jpg] |
| |||||||||

{kind=link}
{kind=link}