 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 123-124 Short Report Craniofacial surgery and optic canal decompression in adult fibrous dysplasia A. K. Mahapatra, P. K. Gupta, R. R. Ravi Department of Neurosurgery, Khoula Hospital, P. O. Box 90, Mina Al Fahal, Postal Code 116, Sultanate of Oman.
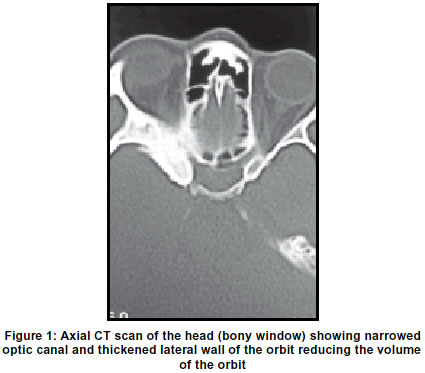
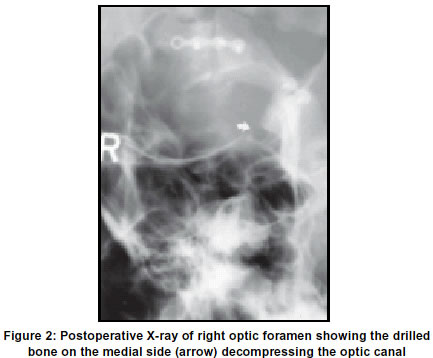
Accepted on 08.10.2001. Code Number: ni03041 A 29-year-old female had a 3-year history of bony swelling over the right frontal area. For 3 months she noticed proptosis of her right eye. Investigations revealed fibrous dysplasia involving the right half of the frontal bone and the right greater and lesser wings of the sphenoid bone. Visual evoked potentials (VEP) showed delayed latencies on the involved side. A craniofacial surgery with optic canal decompression was performed. Follow-up after 2 years revealed normalization of VEP. Key Words: Adult fibrous dysplasia, Proptosis, Optic nerve decompression. Fibrous dysplasia is a rare condition and is reported in 1:4000 10,000 people.1 It is generally believed that the condition is more frequent in children and does not increase after the period of bony growth.2 Rarely, fibrous dysplasia can involve the skull base and orbit, resulting in optic nerve compression and visual loss.3-5 We present a rare case of skull base fibrous dysplasia with proptosis and optic canal compression, in which optic canal decompression was carried out. Case Report A 29-year-old female presented to us with a slowly growing bony swelling over the right frontal area of 3-year duration. For 3 months, she noticed progressive, painless, axial proptosis of her right eye. However, except for mild blurring of vision, she did not have any significant visual complaints. Examination revealed a diffuse bony swelling over the right frontal area and axial proptosis of the right eye. Her vision was normal and her ocular movements were full. Fundus examination revealed pallor of the optic disc on the right side. There was no evidence of neurofibromatosis. Visual field charting showed normal fields. Visual evoked potentials (VEP) using pattern reversal showed significant delay in the P 100-wave latency on the right side. The latency of the left side was normal. CT (computerized tomography) scan demonstrated a significantly thickened and hyperostotic right half of the frontal bone and of the entire right sphenoid wing, consistent with fibrous dysplasia (Figure 1). The right optic canal was significantly narrowed and there was proptosis of the right eye. A bicoronal skin incision was used. The right frontal bone was shaven off using high-speed drill. Right fronto-temporal craniotomy was performed and through an orbitozygomatic approach, the right orbit was de-roofed. The greater wing of the sphenoid and anterior clinoid were also partially drilled out extradurally, using high-speed drill. The right optic nerve was exposed extradurally. The optic canal decompression was restricted to the medial side, as the bone lateral to the right optic nerve was very thick. The dura was opened to assess the degree of optic canal decompression. The bone flaps were replaced and fixed using mini plates and screw. The postoperative period was uneventful. Repeat X-ray of the optic foramina revealed an adequately decompressed optic canal (Figure 2). Discussion Fibrous dysplasia is a rare condition of unknown etiology.1,2,5 Rarely, the disease is also reported in adults.5 In our patient, swelling on the frontal bone was the initial symptom, noticed at the age of 26 years. In orbital fibrous dysplasia, orbital plate of the frontal bone and sphenoid wings are involved.2,6 In our patient, the frontal bone and sphenoid wings were involved. Orbital fibrous dysplasia can present in various ways. More often the patients present with headache and facial asymmetry, due to the enlargement of the facial bones. Painless proptosis is not uncommon. Only rarely, the proptosis is severe.1,2,6,7 Visual dysfunction and optic atrophy occur in lesions involving the sphenoid wing, encroaching upon the optic canal.1,4,5,7,8 Typically, the visual loss is slowly progressive, which could be unilateral or even bilateral.3,7,9 Infrequently, visual deterioration could be rapid, ranging from few hours to a few days.5,9,10 Acute visual loss is probably the result of the vascular event, affecting the ophthalmic artery. Acute visual deterioration can also result from associated pathologies like mucocele5 or aneurysmal bone cyst11 around the vicinity of the optic canal. In a recent publication, Papadulos et al5 reported other associated lesions in both their patient. In one patient, there was a sphenoid mucocele and in the second, MRI revealed a homogenous mass on the right occipital area. The aim of the treatment is to correct cosmetic deformity incurred due to overgrowth of bone or decompression of the neural structure producing symptoms.1,3-5,9 Weisman et al10 reported a case in whom visual loss was reversible. In adults, visual deterioration due to fibrous dysplasia is usually a slow process and occurs over months or years. Optic nerve decompression is a logical option in patients with visual loss. Surprisingly, only 9 cases are reported in the world literature.5,7,9 Our case is the tenth reported adult patient with fibrous dysplasia and visual movement in whom optic canal decompression was carried out.10 Visual improvement has been reported in 7 of the 9 adult patients with acute visual loss.5 We recommend optic canal decompression as the procedure of choice in patients with mild visual deterioration due to fibrous dysplasia. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03041f2.jpg] [ni03041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}