 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
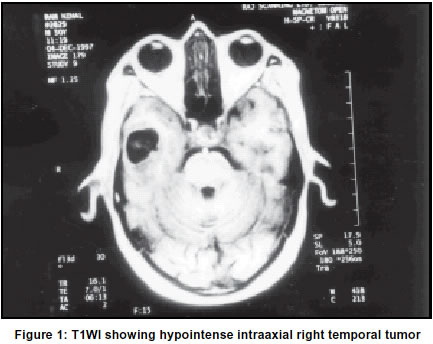
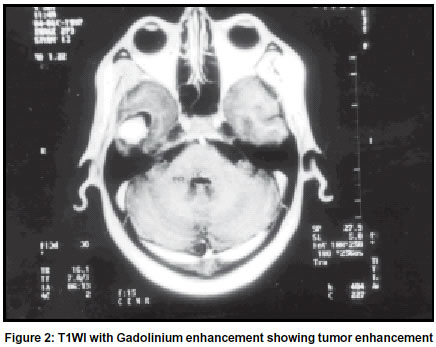
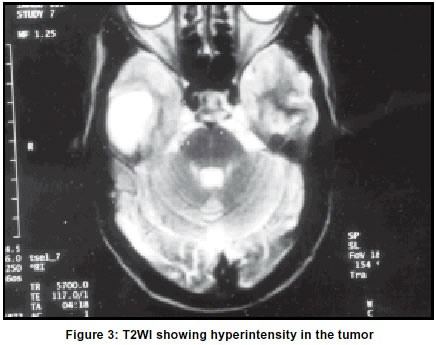
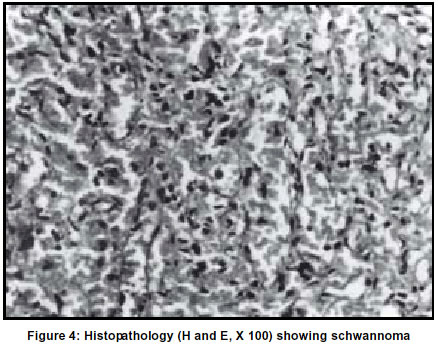
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 125-127 Letter to Editor Intracerebral schwannoma H. S. Bhatoe, K. Srinivasan,* A. K. Dubey Department of Neurosurgery and *Pathology, Command Hospital (Central Command), Lucknow-226002, India. Code Number: ni03043 Sir, Intracranial schwannomas most often arise from the vestibulocochlear nerve and uncommonly from other cranial nerves. Rarely, intracranial schwannomas may not be associated with any of the cranial nerves such schwannomas account for less than 1% of surgically treated schwannomas of the central and peripheral nervous systems.1 We present one such case who presented with seizure disorder. A 50-year-old male was admitted with headache and two episodes of generalized tonic-clonic seizures. There was no aura, and no post-ictal weakness. Neurological examination was unremarkable, and cognitive functions were normal. EEG did not reveal any abnormality. MRI brain showed cystic intracerebral space-occupying lesion in the right temporal pole. The tumor was hypointense on T1-weighted images (TIWI) with bright enhancement on administration of intravenous Gadolinium (Figures 1 & 2). Surrounding cystic component remained hypointense. The tumor was hyperintense on T2-weighted images (T2WI) (Figure 3). The tumor was exposed by right temporal craniotomy. Dural opening revealed distended temporal pole with flattened sulci and gyri. Corticectorny revealed encapsulated, solid relatively avascular tumor, which could be totally excised in one piece. Postoperative period was uneventful. Diagnosis of schwannoma was confirmed on histopathology which revealed a random mixture of Antoni A and Antoni B patterns. Compact bundles of fusiform cells with elongated nuclei and indistinct cytoplasmic borders and Verocay bodies were seen in the Antoni A areas (Figure 4). Major portion of the tumor comprised spindle and polygonal cells randomly dispersed in an open-textured matrix (Antoni B) with focal myxoid and microcystic areas. Hyalinized blood vessels were seen in some areas. Reticulin stain showed a rich pericellular reticulin staining in Antoni B areas. Immunohistochemistry revealed S-100 and vimentin positivity, and EMA and cytokeratin negativity. Intracerebral schwannomas are rare lesions; only 37 well-documented cases have been reported in world literature.2 These tumors commonly arise from the nerve sheaths of peripheral and cranial nerves. However, their intracerebral occurrence is not yet explained satisfactorily. These have been reported in the brainstem and cerebellum as well.3,4 Histogenesis of these tumors is still not settled, and several theories have been proposed for their intracerebral occurrence. These theories can broadly be considered under two groups, the developmental and non-developmental. According to the developmental theory, aberrant schwann cells in the brain parenchyma may occur due to the transformation of the mesenchymal pial cells,5 or from displaced neural crest cells that form foci of schwann cells (`schwannosis').6,7 Relatively young age at presentation also suggests a developmental etiology. Intracerebral schwannomas may occur as part of neurofibromatosis.8 Non-developmental theories base their assumption on the fact that schwann cells are present within the perivascular nerve plexuses and large arteries in the subarachnoid spaces,9 although the existence of these structures deep in the brain parenchyma is doubted.10 However, schwann cells are clearly present in the adrenergic nerve fibres innervating the cerebral arterioles.11 These nerve plexi are common in tela choroidea, which may explain their predilection for periventricular location.12 Intraparenchymal schwannomas are detected either in the first two decades, when they present with an indolent, slow-growing course, or in the elderly, when their symptoms evolve rapidly.2 Males are affected more often and present with headache and seizures. Most of the tumors are located in the supratentorial compartment. On CT the tumors present as isodense or hypodense intra-parenchymal lesions in the frontal or temporal lobes, with a predilection for the periventricular white matter. They show uniform contrast enhancement and often have a cystic component. MRI shows the tumors to be hypointense on TIWI with homogenous high signal intensity on giving intravenous Gd-DTPA. There may be surrounding zone of hypointensity on TIWI and hyperintensity on T2WI due to cerebral edema. These tumors cannot be preoperatively differentiated from other parenchymal tumors. Surgical excision is curative and longterm prognosis is good. Histopathologically, these tumors exhibit the usual features of schwannomas. There are no reported recurrences after excision. H. S. Bhatoe, K. Srinivasan,* A. K. Dubey Department of Neurosurgery and *Pathology, Command Hospital (Central Command), Lucknow-226002, India. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03043f3.jpg] [ni03043f1.jpg] [ni03043f4.jpg] [ni03043f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}