 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
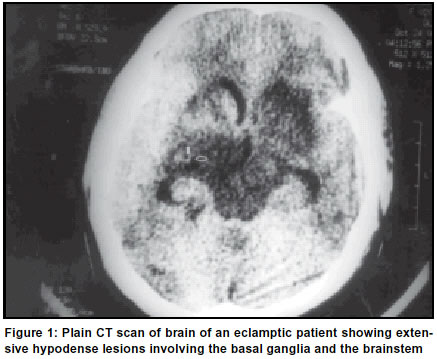
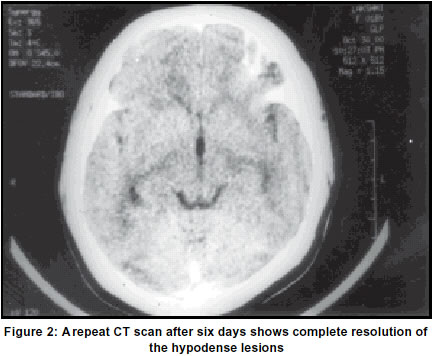
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 127-128 Letter to Editor Unusual radiological picture in eclamptic encephalopathy G. R. K. Sarma, A. Kumar, A. K. Roy Department of Neurology, St. John's Medical College Hospital, Bangalore, India. Accepted on 12.01.2001. Code Number: ni03044 A 20-year-old primigravid lady presented with headache and vomiting of three days duration and three episodes of generalized tonic-clonic seizures followed by altered sensorium in the 35th gestational week. There was no history of fever. She was asymptomatic prior to the present illness. Examination revealed bilateral pedal edema. Blood pressure was 180/130 mm Hg. Uterus was of 32-week size and the fetal heart rate was 142/min. She was in altered sensorium with only minimal flexor response in all limbs to painful stimuli. There was no papilloedema. Extra-ocular movements were full on oculo-cephalic maneuver. There were no meningeal signs. The deep tendon reflexes were exaggerated, more so on the left side. Plantar responses were flexor. Biochemical investigations revealed elevated serum uric acid (6.6 mg/dL) and proteinuria (2 +). Blood urea (24 mg/dL) and serum creatinine (0.6 mg/dL) were normal. A plain CT scan of the brain showed extensive hypodense lesions involving both the thalami, both the basal ganglia and the brainstem (Figure 1). The lateral ventricles were compressed. These lesions were non-enhancing with intravenous contrast administration. There was no evidence of venous thrombosis on the CT scan. She was treated with alpha-methyldopa, magnesium sulfate and mannitol. She delivered a live, pre-term, low birth weight baby (Apgar score of 6). 6 days after delivery, her blood pressure became normal, she became fully conscious, oriented and had no neurological deficits. A repeat CT scan of the brain done at this time was completely normal (Figure 2). Eclampsia is a condition peculiar to pregnant and puerperal women, and is characterized by hypertension, proteinuria, edema and generalized seizures. CT scan in eclamptic patients shows transient abnormalities typically in the posterior regions of the brain namely, the parietooccipital regions (1). Exceptionally, the basal ganglia and the brainstem may show similar lesions.1 MRI also shows hypointense lesions on T1 weighted images and hyperintense lesions on T2 weighted images in the parieto-occipital areas.2 The exact pathologic basis of these lesions is unclear but they probably represent cerebral edema. Focal impairment in cerebral autoregulation is believed to cause vasodilatation and fluid extra-vasation leading to hydrostatic edema.3 Endothelial damage also contributes to the edema.4 Selective involvement of the posterior circulation areas could be explained by their lesser degree of adrenergic innervation supporting circulatory autoregulatory mechanisms.5 The observation that these radiological lesions are completely reversible6 supports the hypothesis that they represent cerebral edema. In severe cases of eclampsia, multi-focal cerebral hemorrhage is seen.7 In our present case, the unusual finding of brainstem and basal ganglionic hypodensities in eclampsia are highlighted. These have to be differentiated from infarcts due to cerebral venous/ sinus thrombosis, which is also common in peri-partum state. Rapid clinical and radiological resolution in our case is a pointer to vasogenic cerebral edema due to eclamptic encephalopathy. G. R. K. Sarma, A. Kumar, A. K. Roy Department of Neurology, St. John's Medical College Hospital, Bangalore, India. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03044f2.jpg] [ni03044f1.jpg] |
| |||||||||

{kind=link}
{kind=link}