 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
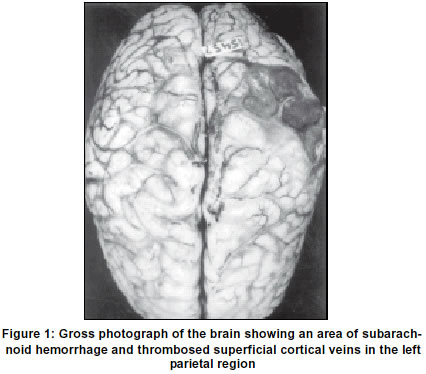
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 128-129 Letter to Editor Aseptic cerebral venous thrombosis associated with abdominal tuberculosis N. Kakkar, A. K. Banerjee, R. K. Vasishta, N. Marwaha,* S. D. Deodhar,** Department of Histopathology, *Department of Internal Medicine, Postgraduate Institute of Medical Edcuation and Research, Chandigarh-160012, India. and **Department of Hematology and Blood Transfusion, Government Medical College, Sector 32, Chandigarh, India. Accepted on 06.02.2001. Code Number: ni03045 Sir, Tuberculosis as a cause of aseptic cerebral venous thrombosis, (CVT) has not been reported in literature. We report here two cases of primary gastrointestinal (GI) tuberculosis (one with dissemination) associated with aseptic CVT. Case 1: A 35-year-old female presented with a 2-months history of diarrhoea, intermittent fever, fatiguability and weight loss. On examination, she was thin-built. The abdomen was distended with a doughy feel and ascites was present. Investigations revealed ESR of 65 mm in the first hour. Four days after her admission she developed impaired speech and memory, delusions, nodding movements of head and irrelevant talking. CT scan revealed right frontal old infarct and a left parieto-occipital infarct. A day later she developed right focal seizures with secondary generalization and right hemiparesis and later died. A complete necropsy was performed. Abdominal organs and lymp nodes showed evidence of tuberculosis. The brain weighed 1070 gm. The left parietal region had an area of subarachnoid hemorrhage (SAH) measuring 5x3 cm. The superficial cortical veins in this area appeared thrombosed (Figure 1). The superior sagittal sinus revealed a thrombus. Bilateral tonsillar and left uncal herniation were seen. On slicing, the left parietal region showed a hemorrhagic infarct measuring 6x4x4 cm corresponding to the area of SAH (Figure 2). Petechial hemorrhages and marked edema were seen around it. The corresponding right parietal region also showed small petechial hemorrhages in the grey matter extending a little into the white matter. Microscopy of the superior sagittal sinus revealed an organizing thrombus (about 3 weeks old). Left parietal region showed a hemorrhagic infarct extending from the pial surface to a variable depth in the white matter. Ball hemorrhages, edema, glial reaction was seen in the white matter surrounding the infarct. Superficial cerebral veins deep in the sulci also exhibited thrombosis. The right parietal region also showed beginning of hemorrhagic infarction. Case 2: A 36-year-old female was admitted with fever, abdominal pain, attacks of intestinal obstruction and loose motions off and on. On examination, she was emaciated. Right axillary lymph nodes were enlarged and matted. Spleen and liver were enlarged, each 3 cm below the respective costal margins. A nodular, freely mobile mass measuring 5x6 cm was felt in the epigastric and right lumbar regions. Bowel sounds were increased. Investigations revealed ESR of 55 mm in the first hour. Three days after admission patient had a generalized tonic clonic seizures lasting for 2 minutes. Two days after the first seizure she had four generalized seizures. Later, the neurologists observed focal seizures involving the right half of the face and upper limits. Complete necropsy was performed. Evidence of tuberculosis was seen in the colon and the various groups of lymph nodes. There was dissemination to the kidney, spleen and liver. The brain showed organizing thrombosis of the superior sagittal sinus, fresh thrombi in cortical veins and fresh hemorrhagic infarct in the left parietal cortex and adjoining white matter. Cerebral venous thrombosis (CVT) could be primary i.e. idiopathic or secondary, which could be either septic or aseptic. Septic CVT is due to bacterial, fungal and parasitic infection. The common causes of aseptic CVT are pregnancy, puerperium, use of oral contraceptives, dehydration, cyanotic heart disease and Behcets disease. Tuberculosis as a cause of aseptic CVT has not been reported before in literature. Pathogenesis of aseptic CVT is either stasis of blood, as the intracranial sinus is a valveless low pressure system or more importantly a hypercoagulable state. This includes an increased number of platelets,1 increase in platelets adhesiveness,1,2 hyperfibrinogenemia3-5 and decrease in fibrinolysis.1,3 Reactive thrombocytosis has been reported in pulmonary tuberculosis.6-8 Baynes et al7 showed in a small number of patients with pulmonary tuberculosis, an increased platelet count and increased platelet aggregability. They attributed this hyperaggregability to a simultaneously increased C reactive protein which has a proaggregating property. Sarode et al9 found significant hyperaggregation in 88% (38/43) patients with intestinal tuberculosis. It can be speculated that a hypercoagulable state does seem to exist in active tuberculosis. This can well be the cause of venous thrombosis. However, more coagulation studies need to be carried out to substantiate this point. N. Kakkar, A. K. Banerjee, R. K. Vasishta, N. Marwaha,* S. D. Deodhar,** Department of Histopathology, *Department of Internal Medicine, Postgraduate Institute of Medical Edcuation and Research, Chandigarh-160012, India. and **Department of Hematology and Blood Transfusion, Government Medical College, Sector 32, Chandigarh, India. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03045f1.jpg] [ni03045f2.jpg] |
| |||||||||

{kind=link}
{kind=link}