 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
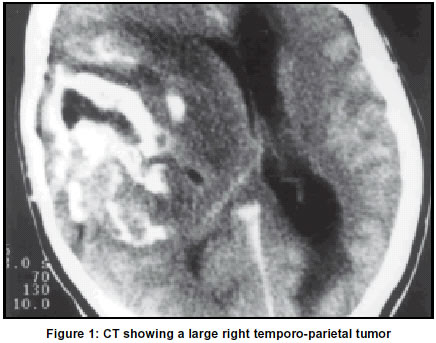
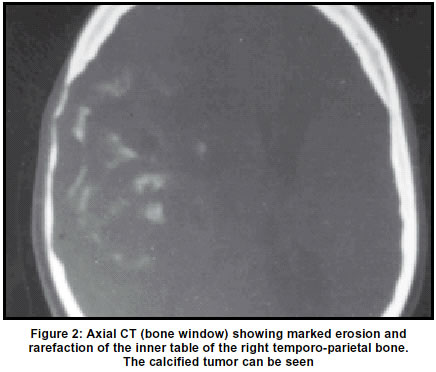
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 129-130 Letter to Editor Oligodendroglioma causing calvarial erosion D. P. Muzumdar, A. Goel, C. K. Pakhmode Department of Neurosurgery, King Edward VII Memorial Hospital and Seth G. S. Medical College, Parel, Mumbai, India. Accepted on 27.03.2001. Code Number: ni03046 Sir Oligodendrogliomas are relatively uncommon primary brain neoplasms and account for 5-7% of intracranial gliomas.1, 2 Calvarial erosion in association with an oligodendroglioma is rare. An extensive and excessive calvarial erosion in a large temporo-parietal oligodendroglioma is described. A 24-year-old female patient, in her sixth month of pregnancy, presented with complaints of gradually progressive generalized headaches and vomiting for the past 3 months. She had decreased vision in the left eye since 15 days. There was no history of fever or tuberculosis. On examination, she was apathic but obeyed simple commands. Vision in the left eye was 6/36. Fundus revealed bilateral papilledema. There was no motor or sensory deficit. Computerized tomography (CT) showed a large right temporo-parietal tumor (Figure 1). There was evidence of subfalcine herniation. The overlying inner table of the temporo-parietal bone was eroded. Bone window showed excessive erosion and thinning of the overlying calvaria vividly (Figure 2). She underwent a right temporo-parietal craniotomy and radical excision of the calcified tumor was performed. The post-operative course was uneventful. The viability of the pregnancy was confirmed in the postoperative period. Histological examination showed features consistent with an oligodendroglioma. At follow-up after 3 months, she was well and delivered a normal healthy child. Oligodendroglioma is a relatively slow-growing primary brain tumor and the diagnosis is usually presented by a long history of symptoms, frequently a seizure disorder or headaches.1, 3 They arise in the white matter and are known to grow towards the cortex. Calvarial erosion is rarely associated with oligodendrogliomas. It is presumed to be pressure erosion predisposed by the peripheral location and slow-growing nature of oligodendrogliomas.4 It is also observed to be independent of the purity or grade of the tumor. Calvarial erosion, in association with the peripheral location of the tumor and calcification is highly suggestive of a diagnosis of an oligodendroglioma. It indicates a lower malignant potential.5 An excessive thinning and rarefaction of the inner table of the tempero-parietal bone secondary to pressure erosion caused by the large size of the oligodendroglioma is vividly seen in the present case. Such profound calvarial erosion in an oligodendroglioma is encountered infrequently in clinical practice. D. P. Muzumdar, A. Goel, C. K. Pakhmode Department of Neurosurgery, King Edward VII Memorial Hospital and Seth G. S. Medical College, Parel, Mumbai, India. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03046f2.jpg] [ni03046f1.jpg] |
| |||||||||

{kind=link}
{kind=link}