 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
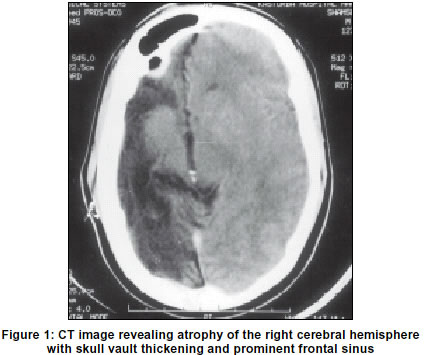
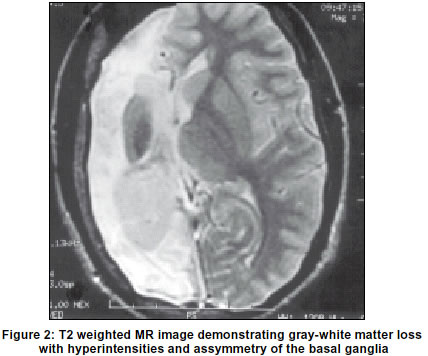
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 136 Neuroimage Dyke-Davidoff-Masson syndrome D. S. Shetty, B. N. Lakhkar, J. R. John Department of Radiodiagnosis, Kasturba Medical College, Manipal, Manipal-576119, India. Code Number: ni03054 A 21-year-old man presented with seizures, behavioral changes and left-sided hemiparesis. There was history of encephalitis at one year of age. Physical examination showed hemiatrophy of the left side of the body with spastic hemiparesis. There were incomplete achievement of mental milestones. Computed Tomographic (CT) scan of brain revealed atrophy of the right cerebral hemisphere with sparing of the basal ganglia.Midline structures were shifted by the intact cerebral hemisphere and skull vault thickening and prominent frontal sinus were noted (Figure 1). Magnetic Resonance (MR) imaging demonstrated the gray-white matter loss with hyperintensities on T2 weighted images and asymmetry of the basal ganglia (Figure 2). Hemiatrophy of one cerebral hemisphere is not frequently encountered in clinical practice. When this develops early in life (during the first two years), certain cranial changes like homolateral hypertrophy of the skull and sinuses occur. The compensatory cranial changes occur to take up the relative vacuum created by the hypoplastic cerebrum. The classical clinical presentation includes seizures, facial asymmetry, contralateral hemiplegia or hemiparesis and mental retardation.1 The clinical findings may be of variable degree according to the extent of the brain injury. Imaging studies show unilateral atrophy of the cerebral hemisphere with ipsilateral shift of the ventricles. The sulci on the involved side are wide and often replaced by gliotic brain tissue. In congenital hemiatrophy, when the insult occurs in-utero, there is shift of midline structures towards the side of the disease and the sulcal prominence replacing the gliotic tissue is absent. 2 This feature differentiates it from cerebral hemiatrophy which occurs in early life. The etiological factor for Dyke-Davidoff-Masson syndrome has been postulated as trauma, inflammation or vascular malformations and occlusions. When the insult occurs in-utero, it could be due to gestational vascular occlusion, primarily involving the middle cerebral vascular territory. A possible etiological relation of cerebral hemiatrophy with febrile seizures has been reported by Garg et al.3 Puri et al have reported an association of schizophrenia with cerebral hemiatrophy.4 In all three cases reported by Sener et al, the cause of cerebral hemiatrophy was middle cerebral artery stroke.2 References
The following images related to this document are available:Photo images[ni03054f1.jpg] [ni03054f2.jpg] |
| |||||||||

{kind=link}
{kind=link}