 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 167-175 Review Article Deep brain stimulation for Parkinson's disease D. Panikar, A. Kishore Comprehensive Care Center for Movement Disorders, Sree Chitra Tirunal Institute
for Medical Sciences and Technology, Kerala.
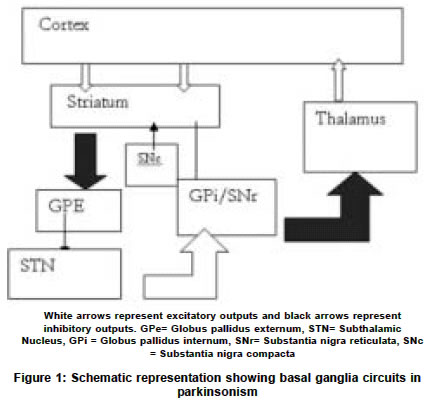
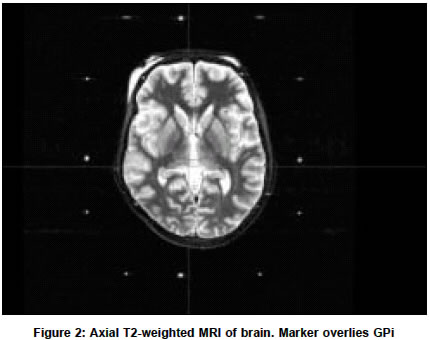
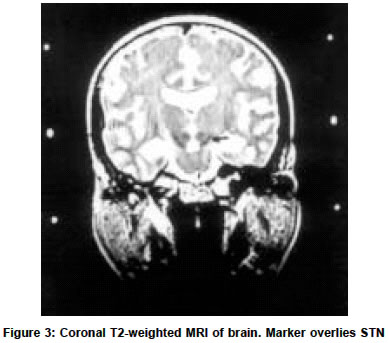
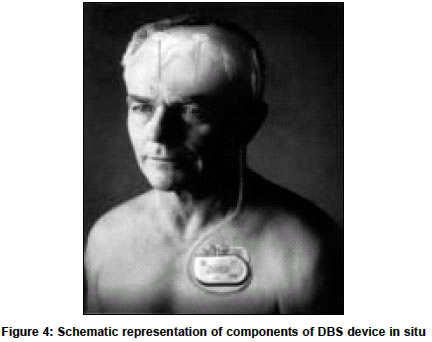
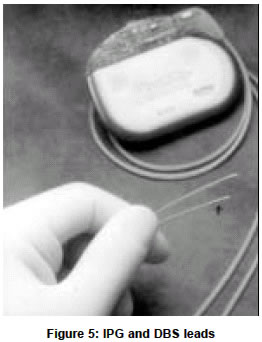
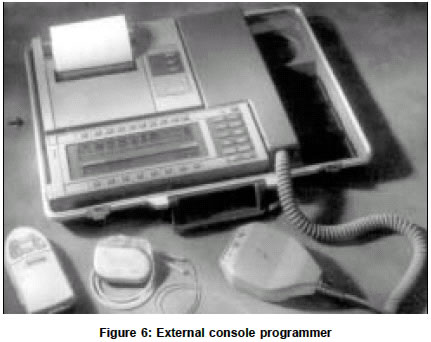
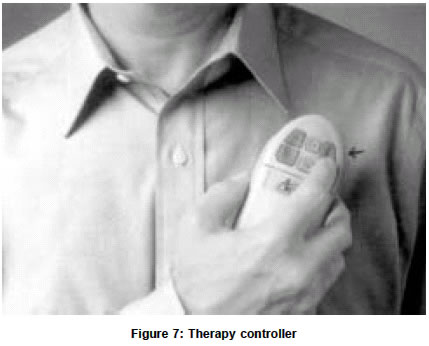
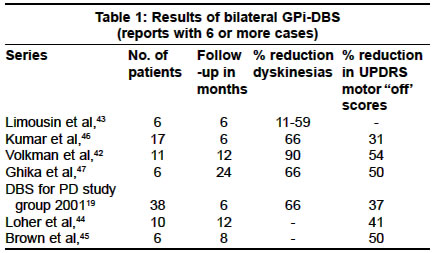
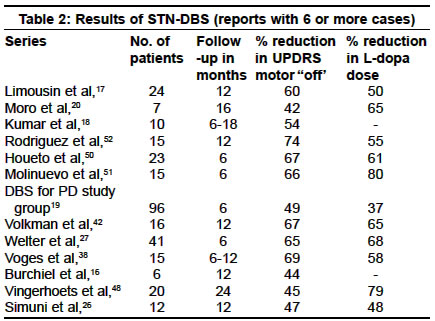
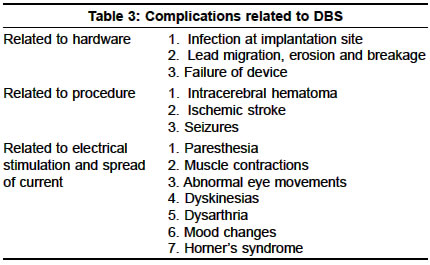
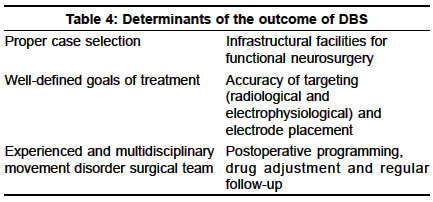
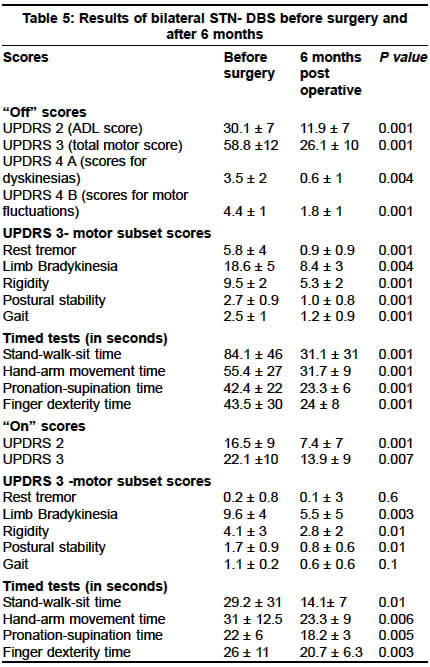
Accepted on 29.06.2003. Code Number: ni03057 Dopaminerigic replacement therapy with levodopa/carbidopa is still the cornerstone for the treatment of Parkinson's disease (PD). However, the medical management of PD is complicated by the appearance of disabling motor response fluctuations, levodopa-induced dyskinesias and psychosis. Since the early 1990s, surgical therapies have made a rapid reentry into the therapeutic armamentarium for PD and deep brain stimulation (DBS) of the globus pallidus interna or subthalamic nuclei is currently the most promising of such interventions. Recognition of the physiological changes in basal ganglia circuits in animal models of PD has provided the much-needed theoretic basis for targeting these areas. DBS of these areas has proven to be a safe procedure and effective against all the major motor symptoms of PD. Though not curative it can substantially reduce motor response fluctuations, levodopa-induced dyskinesias, and improve the quality of life of these patients. DBS is an expensive treatment and hardware-related complications are not rare. The results of the procedure are dependent on careful patient selection and the experience of the performing team. An update on the principles, methods and results of such procedures is essential to raise the awareness of this new therapeutic modality and to provide guidelines to the referring physicians. Key Words: Parkinson's disease, Deep brain stimulation, Subthalamic nucleus, Globus pallidus interna. Introduction Chronic deep brain stimulation (DBS) is currently one of the most promising methods of managing advanced Parkinson's disease (PD). The encouraging results of unilateral posteroventral pallidotomy in controlling motor fluctuations and L-dopa induced dyskinesias (LIDs) played a major role in bringing movement disorder surgery to the center-stage of the management of advanced PD in the early 1990s. In a survey in the USA, 94.3% of neurologists considered refer ring their patients with PD for surgery. Surprisingly, such renewed enthusiasm towards surgical interventions in PD is not seen at present in India, a country that has a long history of functional neurosurgery for movement disorders. A few Indian centers have started performing surgeries for PD including DBS, on a regular basis. A better understanding of the rationale for surgical treatment and a greater awareness of the practice, results and safety of DBS is essential to help physicians guide their patients to explore this new treatment option. Surgeries for PD have become far more effective and safer now because of the scientific rationale for the selection of targets, definition of better clinical criteria for selection of patients, progress in sterotaxic techniques, availability of superior modalities for imaging and intra-operative electrophysiology, and the involvement of multidisciplinary teams trained in the management of advanced movement disorders. A Medline search with the key words deep brain stimulation, Parkinson's disease, subthalamic stimulation, globus pallidus interna and thalamus was used to get the information used in this article. History of DBS The history of DBS in movement disorders can be traced to the 1950s and 60s when early investigators observed that the high frequency stimulation of the ventral intermediate nucleus (Vim) of the thalamus, performed intraoperatively for clinical localization, abolished tremor.1,2 This led to the investigation of the efficacy of chronic stimulation of the Vim nucleus as a treatment for tremor disorders. Chronic DBS of Vim was reported to be an effective treatment for tremor of PD and essential tremor, in the early 1990's.3-5 The success of Vim DBS in PD prompted the application of this technique as the target for pallidotomy, i.e. the posteroventral part of globus pallidus pars interna (GPi) as well as in the subthalamic nucleus (STN).6,7 Many reports have now established that DBS of GPi and STN are both effective and safe in treating medically refractory motor fluctuations and LIDs in PD. Rationale for DBS of STN and GPi A scientific rationale for the choice of surgical targets in PD evolved with the advances in the understanding of the pathophysiology of PD. This was based on the observations from electrophysiological studies in the MPTP monkey model of PD and the effects of lesioning these targets. Such studies proved that there was indeed neuronal hyperactivity in the GPi and STN, secondary to dopamine deficiency, as predicted in the current basal ganglia model for PD (Figure 1).8 The heightened STN activity is a consequence of reduced inhibition from the gobus pallidus externa (GPe), and it causes pathological excitation of the GPi neurons. The pallidal output to the thalamus, which is GABA-ergic, leads to excessive inhibition of the thalamus, thereby reducing the excitatory thalamocortical facilitation of motor cortices. The neuronal overactivity in the GPi and STN has proved to be central to the pathophysiology of parkinsonism. Lesioning these areas leads to marked relief of parkinsonian symptoms in animal models and in human PD. Lesioning and stimulation are presumed to disrupt the abnormal pattern of discharge from these nuclei to the thalamus and help restore normal function in the thalamocortical pathways. Targets for DBS in PD The target in movement disorder surgery refers to the area that is functionally abnormal or the modification of whose activity will result in the alleviation of symptoms. There are 3 targets in the brain, which are effective for DBS in PD. Globus pallidus interna (Figure 2) The posteroventral part of the GPi shows heightened activity and irregular firing patterns in human and animal models of PD. Suppressing this activity by lesioning or high frequency stimulation alleviates parkinsonism and LIDs but the most robust effect is on LIDs.6-13 Within the GPi, there appear to be two different targets .14 Incremental stimulation of the ventral GPi in the "On" state relieves dyskinesias but worsens bradykinesia. On the contrary, similar stimulation of the dorsal GPi in the "Off" state induces dyskinesias, while substantially relieving bradykinesia.14 In DBS of GPi, it is therefore important to choose electrode contacts and suitable current strengths in an intermediate zone, which will relieve both bradykinesia and dyskinesias.14-16 Subthalamic nucleus (Figure 3) STN is the preferred target for DBS in PD according to some experts.15 This view is based on the greater degree of benefits with STN DBS, particularly akinesia, and the reduction in medications permitted by it. 15-20 There is no direct effect of STN stimulation on abolishing LIDs in the short term and it could in fact, worsen dyskinesias unless the dose of L-dopa is reduced concurrently. The reduction in the dose of L-dopa after successful DBS of STN averages around 50% and is thought to be the primary mechanism of the alleviation of LIDs.15-20 Thalamus Intraoperative high frequency stimulation of Vim is highly effective in relieving the tremor in PD.3-.5 In PD, tremor cells are also identified in the STN and GPi. Barring tremor, Vim DBS does not produce a significant change in the other signs of PD and is therefore not recommended for DBS in PD. Mechanism of the action of DBS The exact mechanism of the action of DBS is unknown. As the clinical effects of the DBS of Vim and GPi on tremor and parkinsonism are similar to lesioning, it is proposed that DBS has inhibitory rather than excitation effects on the functions of all its target nuclei. Depolarization block of the neurons of the target nuclei is generally considered to be the most likely mechanism of this inhibition. It has also been proposed that pathological activity such as tremor-related activity in the target neurons may be disrupted (jamming) by high-frequency stimulation.21 There is some evidence to show that high-frequency stimulation of STN in rats and GPi in monkeys, led to decreased firing of neurons from these sites.22-23 In the STN, high-frequency stimulation was found to reduce the firing frequency of its target neurons in the GPi and substantia nigra reticulata (SNr), while low frequency resulted in an increase in activity.23 This is considered as proof that DBS of STN induces a direct inhibition of STN neurons and therefore a reduction in the activity in its target nucleus. STN stimulation has also been shown to increase the activity of the distal thalamic neurons, indicating a release of thalamic neurons from inhibitory GABA-ergic activity. This could be mediated indirectly by reducing the STN-mediated excitation of GPi/SNr. Whether this occurs through reciprocal activation of direct connections between the STN and the thalamus is another speculation. Currently, there is also a thought that DBS may act by different mechanisms in different target nuclei.24 At the usual frequency of thalamic stimulation of 100Hz at 10-ms interval, the second stimulus does not fall in the refractory period of the neuron but in its supranormal period, which is an optimal time for stimulation. Hence, it is doubted whether depolarization blockade is the basic or the only mechanism of the action of DBS in the thalamus. In the GPi, neuronal blockade has been observed only in neurons around the electrode and not in neurons 3 mm away which only showed reduction in firing frequency. Therefore an alternative mechanism of the action of DBS in GPi may be by direct stimulation.24 It has been proposed that GPi and STN stimulation could act by releasing the inhibitory neuro- transmitters from the afferents to them rather than block transmission in its efferents.25 Selection of patients The most important factor that decides the success of DBS is the selection of clinically definite cases of PD who are likely to obtain the greatest degree of benefit from it. At present DBS is recommended only for patients who have been adequately tried on optimal doses of anti-parkinsonian medicines but continue to be disabled from motor fluctuations and LIDs. Earlier surgery may be indicated if there is a risk of loss of job, loss of independent living or of the inability of the individual to perform his or her functions in the family and society. The mean UPDRS motor score (subset 111) in most cohorts that have reported beneficial effects, ranges from 49 to 67 though patients with less severe disease have also been found to show significant benefits.26 Patients who have intolerance to the psychotoxic effects of L-dopa and dopamine agonists (and not due to underlying dementia) or somnolence and mood changes from medications, can also be considered for bilateral DBS of STN. This is because DBS of STN permits reduction in the dose of L-dopa. Age at surgery and duration of disease do not predict clinical outcome but the motor disability tends to improve more in younger patients with shorter duration of disease.27 Preoperative L-dopa responsiveness of symptoms assessed by an L-dopa challenge test, is the most important parameter that helps in the selection of cases.27 The only exception is tremor which will respond well to DBS even if it is refractory to medical treatment. Poor scores for gait and axial structures in the "On" state even with optimal doses of L-dopa and "On" state freezing may predict poor response of these symptoms following DBS. Patients need to undergo detailed clinical examination by a neurologist experienced in the management of advanced PD or by a movement disorder specialist, for confirming the diagnosis of PD, selection of candidates suitable for surgery, for performing the L-dopa challenge test to identify L-dopa responsive and resistant symptoms, and to reliably predict the likely benefits of surgery in individual cases. The definite exclusion criteria for DBS in PD include secondary parkinsonism and parkinsonism plus syndromes. Severe depression and significant cognitive impairment are associated with poor outcome. Significant medical illnesses that are poorly controlled or will jeopardize the lifespan of the patient are relative contraindications. Abnormalities in MRI such as severe cerebral atrophy, multiple infarcts, etc. predict poor outcome. Patients who are not equipped to handle the rigors of a long surgery requiring considerable patient co-operation should not be selected for DBS. Patients who are not willing or are unable to turn up for repeated follow-up or to adhere to the titration schedule of medication adjustment required after DBS may not experience sustained benefits from surgery. Patients and their families need repeated counseling prior to surgery to help them have realistic expectations from surgery. Systematic and objective evaluation and documentation of the benefits of surgery involves the use of internationally accepted protocols such as the Core Assessment Program for Intra Cerebral Transplantations (CAPIT) or Core Assessment Program for Surgical Interventional Therapies in Parkinson's disease (CAPSIT-PD), neuropsychological tests and quality of life scales.28,29 Method of DBS Ideally, DBS surgeries should be performed by a well- trained and experienced team comprising a functional neurosurgeon, movement disorder neurologist, radiologist and if available, a neurophysiologist, and in centers with adequate infrastructure and facilities to perform functional neurosurgery. DBS involves stereotaxic placement of an electrode with 4 active contacts within the target, which is then connected to an externally-implanted pulse generator or IPG (Figures Figure 4 & Figure 5). The most commonly implanted electrodes are quadripolar electrodes with 4 contacts separated by 0.5 mm. The contacts can be activated in the monopolar mode or in the bipolar mode. Implantation of electrodes for DBS is done with the subject conscious during the procedure. The first step in the surgical procedure involves fixing the metal stereotactic frame to the skull under local anesthesia. The second step is the location of the target. In general 2 approaches are used for this purpose (1) imaging with or without computer assistance and intraoperative macrostimulation or (2) imaging with or without computer assistance and microelectrode recording (MER) and stimulation with or without macrostimulation. Ventriculography, CT and MRI scans are used for imaging. As MRI provides greater anatomical resolution, most of the centers prefer it.30 CT scan is used by some to complement the information obtained by the MRI. Geometric distortion in MRI has not been proven to be a practical problem in centers using the Leksell system.31 The Tasker's group from Toronto has compared the accuracy of CT with MRI and found no greater inaccuracies in MRI than CT.32 The third step is intraoperative electrophysiology to confirm the location of the tip of the recording/stimulating electrode in the target and to identify the best location within the target for the placement of the DBS electrode. Both MER and or macrostimulation can be used for electrophysiological localization. It is controversial whether MER is essential for stereotaxic surgery for PD with some authors arguing that MER does not provide added accuracy or clinical benefits in comparison to the use of macrostimulation alone.33 MER techniques are of proven safety though intracranial hemorrhage is more often encountered with it, probably due to the multiple electrode passages required for intraoperative neurophysiological recording.19 A safe alternative is to reduce the number of passages to the minimum required. In the absence of MER, electrophysiological localization can be done by macrostimulation using the probe for radiofrequency lesioning. The final track for the implantation of the DBS electrode is determined by identifying the electrode track that gives the longest run of the target neurons, contains sensorimotor neurons and tremor cells and gives maximum clinical benefit and the least side-effects when test stimulus is given. Once the best location for stimulation is determined, the recording or stimulating electrode is replaced by the implantable multicontact electrode used for DBS. A final test stimulation is done with the DBS electrode. The same procedure is repeated on the opposite side in a bilateral procedure. In the next stage, the external cables of the electrodes are tunneled below the scalp and behind the ear and connected to the IPG, which is usually implanted in a subcutaneous pocket below the clavicle. The latter part of the procedure is performed under general anesthesia. Some centers perform implantation of the pulse generator at a second stage after a gap of few days. Microelectrode recording (MER) in DBS In MER, a fine-tipped electrode is introduced into the brain using a computer-controlled micro-drive mechanism. The microelectrode is connected to an amplifier and recording / analysis system which detects and analyzes neural activity picked up by the electrode as it traverses through the brain towards the target and displays it on a computer screen. The signal is also sent to an audio-monitor and the background noise and electrical activity can be simultaneously heard as they are seen. MER data are collected from 2-4 tracks within the target and are compared to a standard brain atlas, like the Schaltenbrand and Wahren atlas, to determine the exact location of the nuclei. MER in GPi localization The coordinates for GPi are 20 mm lateral to the midline, 3-6 mm inferior to the AC-PC line and 2-3 mm anterior to the mid-commissural line.9 The microelectrode is introduced in the first track based on these coordinates. In PD, the GPe is identified in MER from the two types of neuronal activity seen in it. These are low-frequency discharges with bursts and low-frequency discharges with pauses. The mean firing frequency of GPe neurons is 60 ± 36Hz.34 As the electrode exits the GPe, it enters an area of white matter lamina and border cells, which have a regular firing rate. After traversing this region, when the electrode enters the GPi, there is often an increase in the background noise and multiunit discharges comprising large amplitude spikes, irregular discharge patterns with the highest firing rates among all pallidal cells appear. The mean firing frequency in ventral GPi is 82 ± 32 Hz.35-36 The sensorimotor neurons in GPi show excitatory or inhibitory responses to the passive and active movements of the limbs, axial and orofacial structures. Below the GPi, the cellular activity becomes sparse and the background noise drops. Some centers adopt the technique of entering the optic tract, when there may be an increase in the activity from the optic tract and microstimulation at low current intensities may evoke phosphenes. Identifying the location of the optic tract helps to define the lower border of GPi. The posterior boundary constituted by the internal capsule is defined by making a track through the posterior part of GPi and the capsule is identified as a region of quiet recording. Microstimulation at this area can produce titanic contraction of the contralateral body part. Two to three tracks made in the GPi thus help to identify the posteroventral GPi and the sensorimotor area in it and the DBS electrode can be implanted in the best track defined by MER. MER for STN localization The coordinates for the approximate target in the central region of the STN are usually 12 mm lateral to the midline, 2-4 mm posterior to the mid-commissural point and 3 mm below the AC-PC line.34,37 The trajectory usually encounters the anterior thalamic or thalamic reticular nucleus first. These cells are characterized by spontaneous burst discharges with a mean firing frequency of 8 ± 2 Hz.34 Below the thalamus is a quiet area of the thalamic and lenticular fasciculi with the zona incerta in between. The cells in the zona incerta may have bursting discharges as in thalamic neurons or properties similar to the STN neurons. High-amplitude spikes mark entry into the STN with irregular firing frequencies in the range of 25-45Hz. The neurons in the sensorimotor territory of the STN show modulation in their activity, usually excitatory, with active and passive movements of the limbs. STN may also occasionally show tremor cells. Below the STN is the SNr which is characterized by high-frequency regular firing neurons at a mean rate of 71 ± 23 Hz.34 With the STN spanning around 5-6 mm, the DBS electrode can be placed with its tip at the ventral border of STN such that at least 2 contacts lie within the STN and 1 above it in the zona incerta. Voges and colleagues recently reported that equivalent motor improvement was obtained with electrode locations within the STN, at the dorsal STN-fiber tract interface and close to or within the fiber tracts and or the zona incerta but at lower stimulation energy within the fiber tracts.38 A Japanese group reported that DBS at the dorsal border of STN, which stimulates neurons and their axonal fibers, produced the greatest effect.39 Programming of DBS The pulse generator implanted on the chest wall is externally programmable, so that all the parameters including the stimulation voltage, frequency, electrode contacts and pulse width can be adjusted. The neurologist uses a console programmer to adjust these parameters and obtain an adequate degree of clinical benefits and minimize the side-effects and energy consumption of the IPG battery (Figure 6). In the case of DBS of STN, concurrent reduction of L-dopa is required to eliminate LIDs while the current is stepped up. L-dopa withdrawal has to be done cautiously and under supervision of the neurologist. Patients are also provided with a hand-held device called the therapy controller using which they can make minor adjustments in stimulation parameters, particularly the amplitude of the current, within the limits set by the neurologist (Figure 7). In a recent study, it was shown that the most beneficial effects are obtained at high frequencies and that voltage is the most critical factor that alters STN activity.40 With the standard settings, a battery life of at least 5 years is expected.41 In general, 2-3 visits are required for optimal programming and for adjustment of drugs in the first 6 months of implantation, after which yearly visits generally suffice. Results of DBS in GPi DBS of GPi improves all aspects of parkinsonian symptoms (Table 1) though in some reports the effect of gait and speech are less consistent.42-47 There is a significant reduction in time spent in "Off" following DBS. In the "On" state there is a marked improvement in dyskinesias but not much additional benefit is noted for other symptoms.12,13,19 It received approval for treatment in Europe from 1998. Results of DBS in STN DBS of STN has been shown to improve all motor aspects of PD including gait and axial symptoms.16-20,26,27,38,42,48,50-52 It also reduces treatment-related fluctuations and time spent in `Off" state. LIDs can be effectively controlled when the dose of L-dopa is reduced (Table 2). The safety and efficacy have been established and it has been approved for treatment in Europe since 1998. GPi vs. STN for PD Currently available data are inadequate to decide whether STN is superior to GPi as the target for treatment of PD. Though early reports suggested that DBS of STN might be superior, smaller studies comparing the 2 procedures have not found major differences.16,42,43 Akinesia was found to be better controlled by DBS of STN in one study.15 Volkman and colleagues found that lower energy is required for long-term STN stimulation than for GPi stimulation.42 A large, multi-center, prospective, double blind, non-randomized study showed that both procedures were effective in relieving motor fluctuations and dyskinesias in PD.19 The only striking difference was that DBS of STN permitted a 37% reduction in the requirement of L-dopa. A few studies have shown that DBS of STN can replace L-dopa till the end of the follow up period of at 1.5 to 2 years in 40 to 50% of cases.44,45 Even though DBS of STN permits drug reduction, there are subsets of patients in whom this may be associated with recurrence of mood and speech difficulties which are amenable only to L-dopa therapy. Neither bilateral STN nor GPi DBS affects memory or produces any change in the overall cognitive performance in PD.46 Complications of DBS Adverse effects of DBS are related to the surgical procedure, the implanted device and electrical stimulation of areas adjacent to the target (Table 3). The frequency varies at different centers and depends on the experience of the team to some extent. Serious adverse effects such as death from deep vein thrombosis 4 days following surgery, was encountered in one of the reports.47 Such complications are not unexpected in medically frail elderly patients undergoing any intracranial surgical procedure. Therefore, it is important to highlight such inherent risks extensively prior to surgery. Stereotaxic surgeries carry an inherent risk of intracerebral hematomas (ICH) in the range of 2% to 8% while the rates of ICH reported in DBS range from 0.7 to 2.9% per electrode.48 The risk increases with multiple microelectrode passages in the brain during intraoperative electrophysiology. The number of tracks should preferably be limited to 2-3 per site. In a recent study, long-term hardware-related complications of DBS were reported to be 8.4% which included lead fractures, lead migrations, short or open circuits, lead erosions or infectious foreign body reactions and CSF leak.55 Though improvement in mood has been reported following DBS, others have reported both depression and mania following DBS.19,47-52,54,56,57 These problems were reversible on changing the electrode contacts used for stimulation from lower to higher contacts. Advantages and disadvantages of DBS53 The most striking advantage of DBS is the fact that it does not cause the usual side-effects involving gait, memory and speech associated with bilateral lesioning procedures. Secondly, the stimulation parameters can be adjusted to control the symptoms of PD during follow-up and reduce the side-effects from spread of electric current to adjacent structures. In addition, there is no irreversible destruction of brain tissues involved in DBS. As the integrity of basal ganglia circuits remains intact following DBS, it doesn't preclude the use of any novel future therapy for PD. The major disadvantages are that implanted hardware is expensive (the current cost of the DBS device alone is around 4 lakhs for a bilateral implantation) and the battery needs replacement after about 5 to 8 years. DBS is not a curative treatment and offers only symptomatic benefit and has so far no proven neuroprotective effect in PD. DBS requires life long maintenance. These surgeries can be performed only at centers with adequate facilities and by well-trained multidisciplinary teams, in order to get the best safety and efficacy profile. Patients should be able to report for periodic follow-up and adjustment of medications and stimulation parameters, if required. Management of problems related to hardware can be expensive and can prolong hospital stay. Issues in DBS treatment The results of DBS surgeries are highly dependent on the expertise of the team and the facilities available (Table 4). Indiscriminate application of this treatment to the wrong patient and inaccurate placement of the electrodes can lead to considerable disappointment and financial loss. Regional centers have to systematically document their experience using standardized protocols and critically audit their results to evolve methods for improving the results. In developing countries where only a limited number of patients can afford such surgeries, it may be important that in the early stages, more cases are referred to dedicated centers with trained and highly specialized teams. With increasing experience and understanding of the long- term efficacy of DBS such expertise should be disseminated to establish more centers in a wider area of the country. In PD, it is critical to study whether with disease progression, the appearance of L-dopa-resistant symptoms will overshadow the short-term benefits achieved by DBS which improves only L-dopa responsive symptoms. Theoretically, early introduction of DBS and L-dopa withdrawal could obviate the need for multiple frequent dosing of L-dopa. The pulsatile stimulation by dopaminergic drugs is thought to be responsible for motor fluctuations in PD. However, DBS is not currently recommended early in the illness before patients develop motor fluctuations and dyskinesias and an adequate trial of medical therapy is over. The controversy about the best target for DBS in PD is also yet to be settled.60 The hypothetical neuroprotective role of DBS, based on its ability to reduce STN-mediated glutaminergic stimulation of substantia nigra compacta, is not yet tested in human PD.61 Issues of quality-of-life outcomes and the cost-effectiveness of DBS need to be addressed when studying both short and long-term benefits of DBS. Preliminary reports from the West on these 2 issues are encouraging.62,63 Measures to bring down the cost of these devices and the provision of health insurance cover for DBS in India need immediate attention. Notwithstanding these issues, DBS has undoubtedly opened up a new avenue in the management of advanced PD worldwide and has brought new hope to patients with this condition. Experience of the Comprehensive Care Center for Movement disorders, SCTIMT, Trivandrum The preliminary results of the first 16 cases of STN - DBS for PD at 6 months follow-up are given below. Complications included postoperative seizure in 1 and postoperative confusion in 2. There was no intracerebral hemorrhage or stroke in any, verified by postoperative MRI scans. There was infection of battery implantation side necessitating explantation and re-implantation 3 months later in 1 case. There was possible migration of electrode in another case resulting in loss of benefit seen during intraoperative stimulation, which necessitated re-implantation. The results of the latter 2 cases are not included. In our series, the male to female ratio was 1:1. The mean age at surgery was 55.6 years (SD 11 years), the mean duration of illness was 10.6 years (SD 6 years) and the mean Hoehn and Yahr stage in the `Off" state was 4.1 (SD 0.7). The changes in clinical assessment following DBS are given in Table 5. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03057f4.jpg] [ni03057t5.jpg] [ni03057f5.jpg] [ni03057t1.jpg] [ni03057f3.jpg] [ni03057t2.jpg] [ni03057t3.jpg] [ni03057f2.jpg] [ni03057f6.jpg] [ni03057f1.jpg] [ni03057f7.jpg] [ni03057t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}