 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
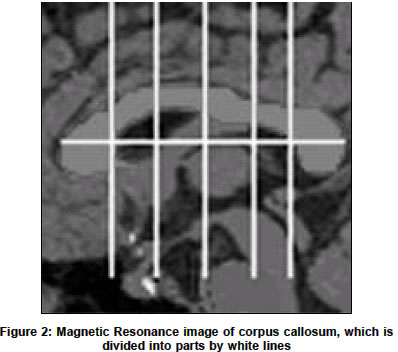
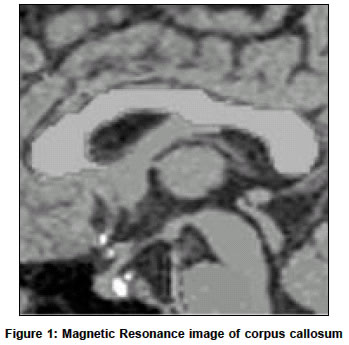
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 189-193 Measuring the corpus callosum in schizophrenia: a technique with neuroanatomical and cytoarchtectural basis G. Venkatasubramanian, P. N. Jayakumar,* B. N. Gangadhar, N. Janakiramaiah, D. K. Subbakrishna,** M. S. Keshavan*** Department of Psychiatry, National Institute of Mental Health and Neurosciences, Bangalore, India.; *Department of Neuroimaging and Interventional Radiology, National Institute of Mental Health and Neurosciences, Bangalore, India; **Department of Biostatistics, National Institute of Mental Health and Neurosciences, Bangalore, India ***Western Psychiatric Institute and Clinic, 3811 O'Hara Street, Pittsburgh, PA 15213-2593 B. N. Gangadhar Accepted on 20.06.2003. Code Number: ni03060 ABSTRACT Background: Corpus Callosum (CC) abnormalities have been described in schizophrenia. Review of CC measurement methods in schizophrenia reveals inconsistency and lack of neuroanatomical basis. Aims: The aims of the study are to describe a new CC measurement method with valid a neuroanatomical and cytoarchitectural basis and to demonstrate inter-rater reliability for the same. Settings and Key Words: Schizophrenia, Corpus callosum, Neuroanatomy, Cytoarchitecture, Imaging. INTRODUCTION Schizophrenia is hypothesized as a neurodevelopmental disorder with regional brain abnormalities.1 Association between corpus callosum (CC) developmental defects and psychosis also supports this view.2 CC size and/or regional CC abnormalities have been described in schizophrenia.3 Many studies have analyzed the morphology of CC in patients with schizophrenia. The majority has found no significant abnormalities in the CC area in schizophrenia. Two have reported an increased size of CC in patients with schizophrenia.4 Many others including a meta-analysis of 11 studies3 have shown that patients have a decreased size of CC. Only a few studies have focused on the regional abnormalities of CC with inconsistent methodology as well as findings.4 Accurate and reliable measurement of the CC poses challenges. Mid-sagittal Magnetic Resonance Imaging (MRI) of the CC area has been used most commonly in studying CC. Considerable variation will be introduced if the slice is off midline and/or at an oblique angle.5 Hence, smaller the slice thickness, more accurate will be the mid-sagittal selection. Objective criteria for the inclusion of the mid-sagittal section also improve slice selection.6 In summary, a review of CC measurement methods in schizophrenia reveals inconsistency and lack of functional basis for subdivision. Very few studies have used a slice thickness of 1 millimeter. We report a reliable, semi-automated CC measuring technique with a neuroanatomical and cytoarchitectural basis tested in a group of 16 never-treated schizophrenia patients using a 1-mm thick mid-sagittal MRI section. MATERIAL AND METHODS The subjects were 16 never-treated, right-handed7, schizophrenia (DSM-IV)8 in-patients. The diagnosis was made using the Schedule for Clinical Assessment in Neuropsychiatry (version 2.1)9 and was confirmed independently by 2 psychiatrists (BNG & NJR). The diagnosis was found to be stable at 6 to 12 months follow-up as re-assessed by one of these 2 psychiatrists. Exclusion criteria were neuroleptic exposure, contraindications to magnetic resonance imaging, history of or current medical illness that may significantly influence CNS function or structure, pregnancy or postpartum (<6 weeks after delivery or miscarriage), seizure disorder, cerebral palsy, mental retardation evaluated by detailed clinical examination, family history of hereditary neurologic disorder that may complicate diagnosis (Huntington's chorea, Wilson's disease), and lifetime history of head injury associated with any of the following: loss of consciousness longer than 10 minutes, seizures, neurodeficit, depressed skull fracture, surgical intervention, and central nervous system infection. Patients provided written informed consent. The Institute's ethic committee approved this study protocol. MRI acquisition Morphometric measurements were conducted blind to clinical data using Scion Image software. The software is in the public domain and was downloaded from the Internet (available at the site: http://www.scioncorp.com). It runs on PC and Macintosh platforms. Measurements from images can be stored separately. This software provides valid and reliable measurements of specific structures using a semi-automated segmentation approach.10 This semi-automated segmentation method to measure volume of brain structures correlated highly with the point-counting stereological approach.10 From the set of T1-weighted three-dimensional MP-RAGE sagittal images, the mid-sagittal section was selected using the following inclusion criteria6: 1) A distinct outline of the CC, 2) An easily identifiable cerebral aqueduct, 3) Clear visibility of cortical gyral crests both anteriorly and posteriorly to the CC, and 4) Absence of visible intrusion into the gray and white matter. All the selected images were inspected and approved by the neuroradiologist (PNJ). The computer using the scion image software automatically calculated all measurements. The desired structure was outlined and measured by the rater using the computer mouse-controlled pointer. The rater (GVS) remained blind to the clinical details. Areas of the intracranium, CC and its parts were measured in the mid-sagittal section in mm2 (Figure 2). In this study, the CC was divided into anterior CC, body, isthmus, and splenium. The software semi-automatically divides the CC based on a neuroanatomical basis.11 Genu and anterior midbody were grouped as anterior CC based on cytoarchitectural principles.12,13 The intracranial area was measured by tracing along the inner table of the skull, above the sphenoid sinus, along the basi-sphenoid, and across the foramen magnum.14 The exact steps of measuring the CC using the scion image software are as follows: The CC in the mid-sagittal section is segmented automatically using the scion image software as shown in Figure 1. A straight line is drawn antero-posteriorly using the scion image software (from the left to right) over the CC passing through the point of maximum curvature of the inner border of the genu. Using the scion image software, four perpendicular lines are automatically drawn on the CC. Finally, the fifth perpendicular line is drawn by the software at the point where the straight line cuts the inner body of the genu of the CC. Now the CC is divided into various parts as shown in Figure 2. To assess inter-rater reliability, two raters (GVS & PNJ (neuroradiologist)) independently rated 16 coded mid-sagittal sections and were blind to the clinical details of the subjects. The neuroradiologist (PNJ) initially trained the rater (GVS) on a few mid-sagittal MRI sections, which were not used in the study. The inter-rater reliability was calculated by intraclass correlation coefficient (ICC). RESULTS The ICC for the various brain measurements were as follows: intracranial area = 0.95; cerebral hemisphere area = 0.86; septum pellucidum area = 0.94; CC area = 0.93; anterior CC area = 0.84; area of body of the CC = 0.83; area of CC isthmus = 0.65; area of CC splenium = 0.88; maximum antero-posterior distance of CC = 0.96; inion-nasion distance = 0.97; maximum antero-posterior internal diameter of the skull = 0.97. DISCUSSION In this study, we have demonstrated a reliable method for measuring the CC. Human and primate studies suggest that various cortical areas are topographically mapped in the CC,15,16 and that regional differences in the fiber composition correspond to this topography.12,13 Areas of the cortex that subserve higher order processing (association areas) tend to project via small axons (<2 mm in diameter), whereas the visual, somatosensory, primary motor and sensory cortices tend to project via large axons (>2 mm in diameter).17 Thin fibers are most dense in the anterior CC 17 that sub serves connections between prefrontal cortices.11 Prefrontal cortical structural abnormalities have been demonstrated in schizophrenia.18 Since the various cortical areas are topographically mapped in the CC,15,16 prefrontal cortical abnormalities could be reflected by anterior CC abnormalities. In this context, the method described in this study becomes relevant in studying the CC in schizophrenia. We used a semi-automated technique in which measuring the maximum antero-posterior distance of CC is the only manual step. Subdividing the CC and measuring the areas by segmentation are computerized and automatic. High inter-rater reliability (ICC=0.96) has been established for the manual step. We are unaware of any other study using a similar technique. In addition, high inter-rater reliability (ICC=0.97) for measures like inion-nasion distance and maximum antero-posterior internal diameter of the skull adds further strength to the inter-rater reliability. Absence of linear correlation has been demonstrated between the brain and constituent regions.19 Hence, to correct the differences in intracranial volume between subjects,18 we suggest that the intracranial area can be used as a covariate rather than ratio method as in prior studies.3 To our knowledge, few earlier MRI studies used a 1-mm section. A thinner slice ensures more precise MR morphometric measure.18 Objectively defined mid-sagittal section, measurement on coded slices, good inter-rater reliability (one of the raters being a neuroradiologist (PNJ) and the other rater (GVS) being initially trained by the former) ensured avoidance of rater bias. Despite these methodological advantages, the measurement of isthmus had moderate reliability. This limitation of our study is probably due to poorly defined isthmus. In this study, we have demonstrated a reliable, semi-automated, computerized method for measuring the CC using a 1-mm thick mid-sagittal MRI section in never-treated schizophrenia patients. This method has a neuroanatomical and cytoarchitectural basis, which is relevant for schizophrenia research. The software used in this study is user-friendly and is available in the public domain on the Internet. Thus, the methodology demonstrated in our study is simple, relevant and reliable, and it can be used for future schizophrenia research. REFERENCES 1. Keshavan MS. Neurodevelopment and schizophrenia: quo vadis? In: Keshavan MS, Murray RM, editors. Neurodevelopment & Adult Psychopathology. London: Cambridge University Press; 1997. pp. 267-77.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03060f2.jpg] [ni03060f1.jpg] |
| |||||||||

{kind=link}
{kind=link}