 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
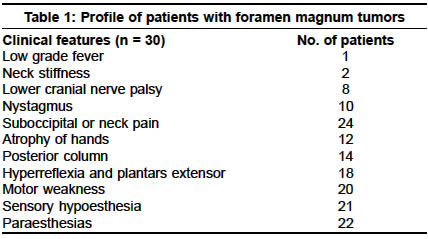
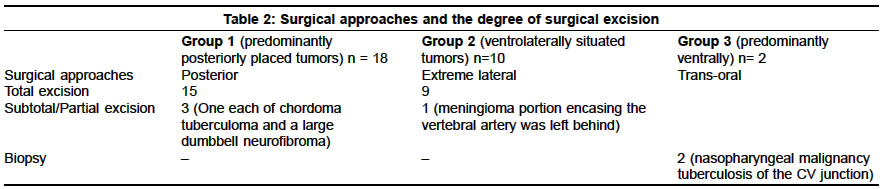
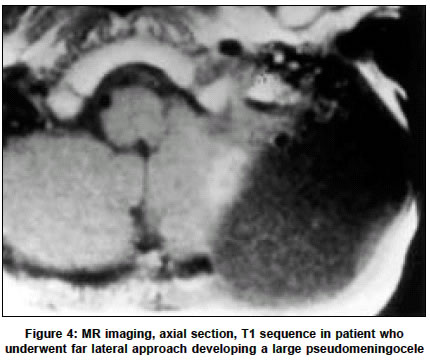
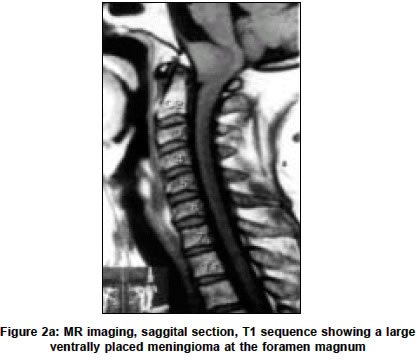
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 193-196 Foramen magnum tumors: A series of 30 cases P. Sarat Chandra, A. K. Jaiswal, V. S. Mehta Department of Neurosurgery, AIIMS, Ansari Nagar, New Delhi-110029, India. P. Sarat Chandra Accepted on 04.08.2002. Code Number: ni03061 ABSTRACT Background and Aims: Foramen magnum tumors, especially those located ventrally, are surgically challenging. We studied clinical and surgical details of extramedullary tumors located in the region of the foramen magnum. Key Words: Foramen magnum, Craniovertebral junction, Tumors, Complications. Foramen magnum tumors, especially those located ventrally, are surgically challenging. Their location, combined with their close anatomical relation to critical vascular and neural structures makes radical tumor resection difficult.1-7 The approach for a foramen magnum tumor is decided by its location. Posteriorly or posterolaterally situated tumors may be approached through a posterior route. Ventrally or ventrolaterally situated tumors can be approached through an extreme lateral approach.7 MATERIAL AND METHODS This is a retrospective analysis of 30 patients having extramedullary tumors located in the region of the foramen magnum, operated over 8 years between January 1993 and December 1999 in the neurosurgery department at the All India Institute of Medical Sciences, New Delhi. RESULTS There were 18 males and 12 females. The age ranged from 13 to 75 years (mean 38 years). The clinical profile included sensory symptoms or signs in 22 patients, features of myelopathy (either weakness, hyperreflexia or plantar extensor) in 24 patients, lower cranial nerve weakness in 8 and sphincter disturbances in 6 patients (Table 1). Other clinical features included small muscle atrophy in 12, suboccipital neck pain in 24, nystagmus in 10 and neck stiffness in 2 patients. MR imaging revealed a predominantly dorsally situated tumor (Group 1) in 18 cases. These included 10 neurofibromas, 4 chordomas, 2 hemagiopericytomas, 1 angiomatous meningioma and 1 tuberculoma. Of the 10 neurofibromas, 6 were located predominantly dorsally and could be excised through a standard posterior approach. Four tumors had a posterolateral location and maneuvers like removing the C1 arch more laterally and incising the dura in a T-shaped manner had to be performed. Of these, 2 tumors had a dumb-bell extension into the lateral cervical region and in 1 case an additional lateral cervical approach had to be performed for tumor resection. The 4 chordomas were located laterally in the extradural plane and in 1 case there was destruction of the facet joint. Total resection of the chordomas could be performed in 3 cases. In 1 case there was extensive occipital bone and lateral mass bone destruction and a subtotal resection was performed. The craniovertebral region was subsequently fixed posteriorly with a contoured rod. All the tumors were located in an anterior and lateral plane and there was severe cord compression in each case. The tumor could be accessed through a posterior approach in all the cases. Both the hemagiopericytomas and the angiomatous meningioma presented as small intradural extramedullary lesions and could be excised by the posterior route. The tuberculoma was seen on MR imaging as a well-defined extramedullary intradural lesion. During surgery the lesion was firm in consistency and did not have a good plane of cleavage. Frozen section confirmed a tuberculoma, and only a partial resection of the tumor was done. There was no mortality in Group 1. One patient with a large chordoma destroying the facet joint developed transient worsening of neurological deficits after surgery, but this improved completely on follow-up. A second group of patients (Group 2) had ventrolaterally situated tumors (n = 10) which were surgically accessed by an extreme lateral approach. This group consisted of 8 meningiomas and 2 chordomas. A third group (Group 3) of patients consisted of cases in which the tumors were located anteriorly (n= 2). One patient had a large tuberculous lesion which had destroyed the dens and anterior arch of atlas and caused cord compression. The other patient had a nasopharyngeal malignancy involving the anterior part of the foramen magnum. Both these patients underwent a transoral biopsy. The patient with tuberculosis underwent an additional posterior fixation with a contoured rod. Table 2 summarizes the extent of tumor resection in each case in the 3 groups. Two patients died. One patient with a foramen magnum meningioma developed lower cranial palsy after a total tumor excision and subsequently succumbed to aspiration pneumonitis (Group 2). The other patient, having a nasopharyngeal malignancy (Group 3) underwent trans-oral biopsy, developed wound dehiscence and septicemia and subsequently died. Other complications included CSF leak in two patients, one belonged to Group 1 and the other to Group 2. In both cases, the leak was controlled with serial lumbar drainage of CSF. One patient with a large foramen magnum meningioma developed a psuedomeningocele (Figure 4), necessitating the need for a thecoperitoneal shunt. Other complications included laryngeal edema, transient worsening of neurological deficits, and stitch abscess. The follow-up period ranged from 4 months to 6 years (mean of 3.5 years). Four patients were lost to follow-up after an initial follow-up at 1 month. Of the 28 surviving patients, 20 had complete recovery in their neurological deficits and could get back to their occupations. Four patients had partial improvement in their neurological status. DISCUSSION A variety of pathological lesions may occur at the level of the foramen magnum. However, meningiomas and neurofibromas are the commonest.5,6 In a recent study, about 70% of the lesions at the foramen magnum were meningiomas or neurofibromas.7 In the present study about 60% of the cases were either meningiomas or neurofibromas. The clinical profiles of the patients with foramen magnum tumors are varied and include neck pain, dyesthesias, cruciate hemiparesis, and pseudoathetoid movements of the upper limbs.8-12 However, there are no definite clinical markers for foramen magnum lesions. The commonest clinical features in our series were suboccipital neck pain, paraesthesias and pyramidal tract involvement. The surgical approach to these lesions would depend on their anatomical location. In general, anteriorly placed lesions may be accessed through a trans-oral route. However, this route is usually suitable only for extradural lesions. The route is also suitable for biopsy of the lesion or for limited tumor resections. Some authors have described this route for the removal of intradural lesions like ventrally situated meningiomas.5 However, the risks of CSF leak and infections limit the use of this approach. The lateral approaches to anterolaterally placed lesions are technically challenging but are effective in providing a wider exposure suitable for excising lesions in this area. A posterior approach or a lateral suboccipital approach may not be suitable to access the lesions in this region.13 Various names have been given for the far lateral approaches, including lateral approach,14 lateral inferior suboccipital approach,15 transcondylar approach, and the extreme lateral transcondylar approach.17,18 We have found the extreme lateral approach satisfactory for all our Group 2 cases. The main disadvantages of this approach include the possibility of vertebral artery laceration during the exposure, CSF leak and occipitocervical instability if the entire occipital condyle is resected.19 The incidence of CSF leak was significantly reduced in our series after the routine use of fibrin glue. We observed that the application of the glue to the fascial patch and its placement over the site of the dural defect is an effective technique to avoid CSF fistula. Opening of the dura posterior to the site of entry of the vertebral artery, rather than around the artery as has been described by some, was an effective technique. By using this technique, the entire vertebral artery along with the dura could be reflected anteriorly and the operative field was exposed widely. The closure of the dura could then be done by direct suturing. We found that the microdoppler was an effective instrument and helped in avoiding injury to the vertebral artery. This instrument helped in locating both the intradural and extradural vertebral artery and also helped in identifying the artery encased within the tumor. It was observed that it was unnecessary to resect the occipital condyle and more often the tumor itself creates space for dissection. The extent of surgical excision will depend on the site, size and nature of the tumor and more importantly on the experience of the operating surgeon. Samii in a series of 38 patients of foramen magnum meningiomas demonstrated total excision in 80% of meningiomas. Only a subtotal or a partial excision could be performed in all cases with en plaque extension in his series. Similarly, the incidence of total excision was only 31% in cases when the vertebral artery was encased by the tumor.22 In the present series, total excision could be performed in all our cases except in one where the vertebral artery was encased completely and a small portion of the tumor around the artery had to be left behind (Figure 2). Foramen magnum tumors have long been regarded as difficult lesions both in terms of diagnosis and management. However, with the availability of MR imaging, newer surgical techniques and skull basal exposures, the excision of these lesions is becoming easier and safer. REFERENCES 1. Guidetti B, Spallone A. Benign extramedullary tumors of the foramen magnum. Surg Neurol 1980;13:9-17.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03061f4.jpg] [ni03061f3.jpg] [ni03061f2a.jpg] [ni03061f1b.jpg] [ni03061t2.jpg] [ni03061t1.jpg] [ni03061f1a.jpg] [ni03061f2b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}