 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
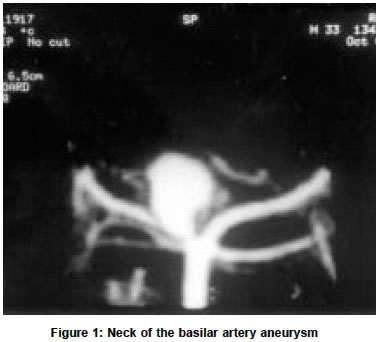
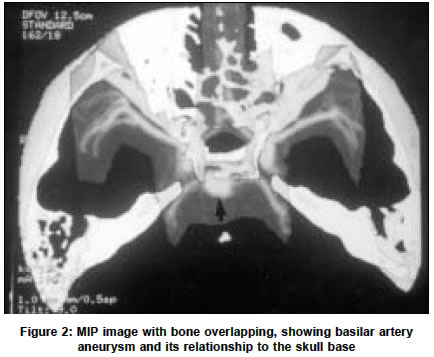
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 206-207 Three-dimensional CT angiography in the evaluation of cerebral arteries in acute hemorrhage K. V. Rajagopal, B. N. Lakhkar, D. K. Acharya Department of Radio Diagnosis & Imaging, Kasturba Medical College, Manipal-576119, Karnataka, India. B. N. Lakhkar Accepted on 27.03.2002. Code Number: ni03064 ABSTRACT Objective: We conducted this study to demonstrate the value of non-invasive three-dimensional CT angiography (3D CTA) in the detection of a cerebral aneurysm. Key Words: Cerebral aneurysm, Computed tomography, Subarachnoid hemorrhage. Acute subarachnoid hemorrhage secondary to aneurysm has a high fatality rate of up to 50%.1,2 Much of the poor outcome is caused by rebleeding.1,2 Three-dimensional CT angiography (3D CTA) may be an alternative to the conventional DSA.3 MATERIAL AND METHODS Fifty non-consecutive patients (28 men and 22 women with mean age of 53 years) with clinical suspicion of SAH were subjected to 3D CTA. Patients who were unstable were subjected to 3D CTA after sedation. Out of 50 patients, 46 patients had SAH as seen on plain CT scan. In the remaining 4 patients SAH was detected by positive CSF finding. Five patients with previously clipped aneurysm were assessed during follow-up examination and were not included in this study. 3D CTA data were obtained using a Wipro GE Prospeed Sx helical CT scanner. The scan volume extended from 2 mm below to 4.8 cm above the base of the sella. The scan plane was kept parallel to the orbitomeatal line. The technical parameters of CT angiography were as follows: rotation 1 per second, collimation 1 mm, tables speed 1 mm/sec, reconstruction interval 0.5 mm, 120 kVp, 160 mAs and field of view (FOV) 16 cm. Using pressure injector (Nemoto), 100 ml of non-ionic contrast media (300mg I/ml, Iohexol) was injected at the rate of 3.5 ml/sec with scan delay of 20 seconds after onset of injection. The results of 3D CTA in patients who were found to have aneurysms were followed up and confirmed by surgical findings. RESULTS The predominant presenting complaints included headache in 32 patients, loss of consciousness in 11 patients, seizures in 4 patients, neurological deficit in 4 patients and third cranial nerve palsy in 1 patient. Out of 50 patients, a total of 39 aneurysms were present in 37 patients. 3D CTA revealed 38 aneurysms in 36 patients. In 1 patient with small ACoA aneurysm, measuring 2.5 mm in size, 3D CTA was non-conclusive and the DSA confirmed the presence of the aneurysm. 3D CTA showed a single aneurysm in 34 patients and double aneurysms in 2 patients. All these 37 patients underwent surgery and the findings on the 3D CTA were confirmed in 36 patients. 3D CTA showed normal study in 14 patients. In all these patients DSA was performed. DSA showed normal findings in 13 of these patients and detected a 2.5 mm aneurysm in 1 patient. During the operation, the site of the aneurysm was correctly predicted in 37 of the 38 aneurysms detected on 3D CTA. In 1 patient, during surgery, an internal carotid artery (ICA) aneurysm was detected at the origin of the ophthalmic artery. The patient in this case was inadvertently interpreted as having a posterior communicating artery (PCoA) aneurysm on 3D CTA. In our study there was a middle cerebral artery (MCA) bifurcation and trifurcation aneurysm in 15 patients (38%), an AComA aneurysm in 10 patients (% ?), and an ICA aneurysm at the origin of PCoA in 9 patients (23%), 2 aneurysms were at the distal anterior cerebral artery (ACA) (5%), 2 aneurysms were at the apex of the basilar artery (5%) (Figures 1 & 2) and 1 aneurysm was located at the carotid_ophthalmic artery junction (3%). The neck of the aneurysm was demonstrated in 37 out of 38 aneurysms. In one large aneurysm at the PCoA, the neck was not clearly demonstrated. There was evidence of calcification of the aneurysm in one patient and thrombus in one other patient. The surgical anatomy was well delineated by 3D CTA. The exact size of the aneurysm, its shape, irregularities of lobulations and relationship to the bone structures were depicted by 3D CTA. DISCUSSION Several recent studies have proposed 3D CTA as an alternative to DSA.4,5 In our study all the 36 patients in whom 3D CTA revealed aneurysms could be directly taken up for surgery without DSA. MIP is less dependent on the user, both the vessels and the neighboring anatomic structures are clearly visible and the picture quality resembles DSA. 3D-CTA has the potential to depict additional information of the relationship to the bony landmarks. Also vessel-to-vessel relations, which vary considerably, were simultaneously projected in CTA. In the majority of the series, the sensitivity of 3D CTA varies from 96 to 100%.4-12 The acquisition time of images on CTA in helical mode is very short and so superior to magnetic resonance angiography and is thus useful in uncooperative or comatose patients. The existence of surgical metallic clips in patients who previously underwent surgery does not significantly hinder 3D CTA evaluation. In conclusion, CTA is a simple, quick, safe, non-invasive, and sensitive modality for the evaluation of intracranial aneurysms and may be a good alternative to DSA. REFERENCES 1. Broderick JP, Brott TG, Dulder JE, Tomsick T, Leach A, Initial and recurrent bleeding are the major causes of death following subarachnoid haemorrhage. Stroke 1994;28:1342-7.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03064f1.jpg] [ni03064f2.jpg] |
| |||||||||

{kind=link}
{kind=link}