 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
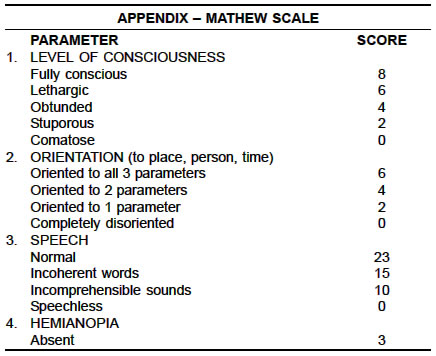
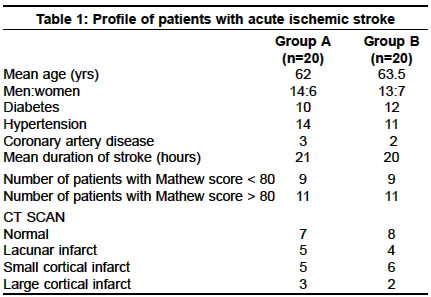
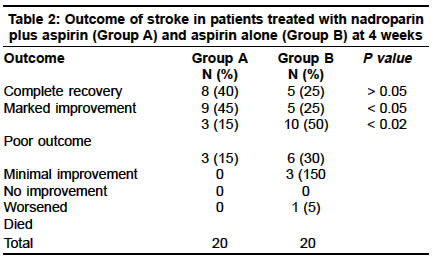
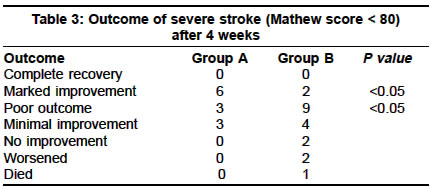
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 208-210 Nadroparin plus aspirin versus aspirin alone in the treatment of acute ischemic stroke G. R. K. Sarma, A. K. Roy Department of Neurology, St.John's Medical College Hospital, Bangalore, India. G. R. K. Sarma Accepted on 16.2.2002. Code Number: ni03065 ABSTRACT Low-molecular-weight-heparin (LMWH) has been widely used in the treatment of acute ischemic stroke but controlled trials are few. In this study, 40 patients with acute ischemic stroke of less than 24 hours duration were randomized to receive either aspirin (325 mg/day) alone or aspirin (325 mg/day) plus subcutaneous nadroparin 4100 units/day. At the end of 4 weeks, the morbidity and mortality were significantly less in the nadroparin group as compared to the aspirin group. There was no increased risk of clinically significant intracranial hemorrhage in either group. The combination of aspirin and LMWH deserves to be tested in larger studies. Key Words: Ischemic stroke, Nadroparin, Heparin. INTRODUCTION Heparin has been used in the treatment of acute ischemic stroke for decades but its use remains controversial.1 The recently concluded international stroke trial (IST)2 found that the benefits of heparin in terms of reduction of recurrent stroke were offset by an identical increase in the number of hemorrhagic strokes. The use of heparin in special circumstances like progressive stroke,3 partial stroke,4 cardio-embolic stroke5 and vertebro-basilar syndromes6 is still debated. Recently, low-molecular weight heparins (LMWH) have been introduced in clinical practice with a number of theoretical advantages.7 However, very few randomized studies are available to assess their utility in acute stroke.8 A combination of aspirin and LMWH has so far not been tested in the treatment of acute ischemic stroke, though the combination of aspirin and un-fractionated heparin was tested in the IST and was found to have no added benefits than aspirin alone. In the present study, a combination of aspirin and a low dose of LMWH nadroparin, was tested against aspirin alone in acute ischemic stroke. The rationale of this combination is that the different mechanisms of the action of aspirin, which targets the platelets, and LMWH, which targets the coagulation cascade, could provide added benefits than either agent alone. MATERIAL AND METHODS This is a prospective randomized trial. Forty patients with acute ischemic stroke of less than 24 hours duration were randomized, by a computer-generated randomization table, to receive either a combination of subcutaneous nadroparin 4100 units and aspirin 325 mg per day (Group A) or aspirin 325 mg per day alone (Group B). Nadroparin was stopped after 10 days of therapy and aspirin was continued. All patients were evaluated at admission with non-enhanced CT scan. Patients with hemorrhagic infarction, active peptic ulcer, recent head trauma or hemorrhagic stroke in the preceding 3 months, gastrointestinal or urinary tract hemorrhage in the preceding 3 weeks or with a blood pressure greater than 185/120 mm of Hg were excluded from the study. Objective assessment of the neurological status was performed and monitored for 4 weeks using the Mathew scale9 (see appendix). In case of clinical deterioration, a CT scan was repeated to exclude hemorrhagic transformation. At the end of 4 weeks, the outcome of the two groups was compared. Statistical analysis was performed by the student's t-test for discrete variables and a p-value of less than 0.05 was accepted as statistically significant. RESULTS There were 20 patients in each treatment group. The two groups were comparable at admission with regards to clinical and radiological parameters (Table 1). At the end of 4 weeks, 40% of the patients in Group A made a complete recovery as against 25% in Group B (Table 2). Marked improvement, defined as that which allowed independence in activities of daily living, was noted in 45% patients in Group A and 25% patients in Group B. This difference was statistically significant (Table 2). 45% patients in Group B as against 15% in Group A, had severe disability due to either minimal or no recovery. This difference was also statistically significant. One patient in Group B died due to progressive infarction while there were no deaths in Group A. No patient in this study had clinically significant hemorrhagic transformation of the infarct. One patient in Group A had mild upper gastrointestinal hemorrhage on the 8th day of therapy and it subsided after withdrawing nadroparin. Even when the analysis was restricted to those patients with severe stroke (Mathew score < 80), the outcome was more favorable in Group A than in Group B (Table 3). DISCUSSION Nadroparin is a LMWH whose mechanisms of action10,11 include not only anti-thrombotic action by virtue of its anti Xa activity, and anti-IIa activity, but also fibrinolytic action by increased plasminogen activator levels, release of tissue factor pathway inhibitor, release of tissue palsminogen activator , and also hemorrheological effects by increased platelet membrane fluidity and blockade of cell surface receptors for platelets. It has a number of advantages over un-fractionated heparin including once or twice a day dosing, predictable anti-thrombotic effect, lack of thrombocytopenia,12 lack of the white-clot syndrome and lack of the need for rigorous monitoring of coagulation parameters. The main drawback of the LMWH is the high cost, which is several times more than that of the un-fractionated heparin. However, this is partially compensated by the lack of the need to monitor coagulation parameters. Previous studies on LMWH did not show significant benefit in acute stroke, except in Kay's study.8 In this study, 306 patients who presented within 48 hours of the onset of stroke were randomized to receive either high or low dose of nadroparin or placebo for 10 days. No significant difference in the primary outcome, namely, death or dependency, was found at the end of 3 months. However, at 6 months, there was a significant dose-dependent reduction in the percentage of patients left dead or dependent in favor of high-dose nadroparin. There was no significant difference between the two groups with regard to hemorrhagic transformation or systemic bleeding complications. In contrast, in a systematic review of all the randomized trials which investigated the efficacy and safety of LMWH in acute stroke, myocardial infarction, venous thrombo-embolism and unstable coronary syndromes, it was found that there were no beneficial effects of LMWH in acute stroke as compared to placebo, while the risk of major bleeding was increased.13 In the TOAST study, synthetic heparinoid ORG 10172 was compared to placebo in acute ischemic stroke of less than 24-hour duration and was found to be superior to placebo. Unfortunately, this study did not address the question whether ORG 10172 has any added benefits over and above aspirin alone.14 In the present study, it was found that a combination of nadroparin and aspirin had improved the outcome of stroke patients when started within 24 hours of the onset of the stroke. More patients on combination therapy made complete or significant recovery. Total lack of improvement or worsening was seen more often in patients on aspirin alone than in the combination therapy group. Beneficial effects were seen even in those patients with severe stroke. There was no increased risk of hemorrhagic transformation with the doses used in this study. It should be noted that the previous studies on heparin and LMWH have used a wide window period of up to 48 hours, which could have negated many of their beneficial effects. It is possible that if the window period is reduced to 12 hours or even less, the beneficial effects would be more apparent. For instance, in the NINDS trial,15 beneficial effects of rtPA were seen only when a narrow window period of 3 hours was used. Probably, LMWH and un-fractionated heparin, like rtPA, deserve another chance to prove their efficacy by using such narrow window periods. In this study, only small doses of nadroparin were used due to the fear of increasing the risk of hemorrhagic transformation due to the combination with aspirin. However, such a combination appears to be safe and trials using higher doses of nadroparin with the hope of further improving the outcome may be justified. The main drawbacks of this study are the small sample size and the short duration of follow-up. Any reasonable conclusion about the efficacy of a drug in a disease like stroke requires study of thousands of patients. However, small pilot studies of this nature provide a direction in which larger trials may be undertaken. The message from this study is that a combination therapy of aspirin and LMWH, instituted in the earliest stages of stroke deserves to be tested against aspirin alone in larger randomized trials. REFERENCES 1. Adams H, Brott T, Crowell R, et al. AHA Medical/ scientific Statement: Guidelines for management of patients with acute ischemic stroke: A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1994;25:1901-14.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03065t3.jpg] [ni03065a1.jpg] [ni03065t1.jpg] [ni03065t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}