 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
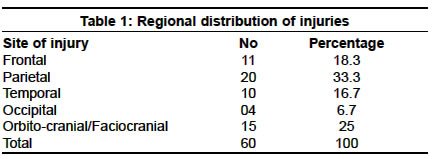
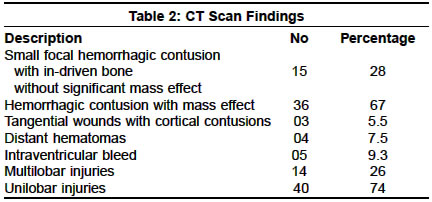
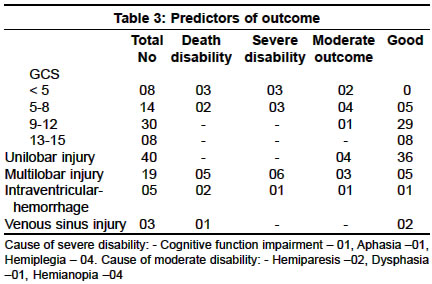
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 215-219 Missile injuries of the brain: Results of less aggressive surgery P. Singh Classified Specialist, Neurosurgery, Army Hospital (R&R) Delhi Cantt-110010. Prakash Singh Accepted on 10.09.2001. Code Number: ni03067 ABSTRACT Sixty cases of missile injuries (59 males, average age 25 years) were studied over a period of one year. Forty-three patients had suffered splinter injuries, 12 had gunshot wounds and 5 had suffered injuries from improvised explosive devices. The Glasgow coma scale was <5 in 8 patients, 5-8 in 14, 8-12 in 30 and 13-15 in 8 patients. Extensive comminution of skull bones was found in 10 patients. Thirty-five patients had penetration of the skull and the rest had orbito-cranial or facio-cranial wounds. CT scan revealed small hemorrhagic contusion with in-driven bones without mass effect in 15, contusion with mass effect in 36 cases, cortical contusions without in-driven bones (tangential injuries) in 3, distant intracranial contusions in 4, intraventricular hemorrhages in 5, multilobar injuries in 14, and unilobar injury in 40. Fifty-two patients were operated upon at our center, of which 30 were operated within 24 hrs, 10 between 24 to 48 hrs, and 12 between 48 to 72 hrs. Six patients were treated conservatively and 2 underwent only a simple closure of scalp wound. Craniectomy was done in 10 and craniotomy in 42 patients. Two patients developed wound sepsis, one had aspiration pneumonia, one had septicemia and one had deep vein thrombosis while one had post-traumatic hydrocephalus. On follow-up at 6 months, the outcome as per the Glasgow outcome scale was as follows: Good outcome in 42, moderate disability in 7, severe disability in 6 and death of 5 patients. Retained bone fragments were found in 36.3 % on follow-up CT scan but no one had brain abscess. Key Words: Missile injury, Cerebral contusion, Skull bone fracture, Glasgow-coma scale. INTRODUCTION Since the invention of gunpowder and firearms, missile injuries of the brain have become unavoidable consequences of military conflicts. The literature is replete with the efforts of neurosurgeons towards treating these injuries. Harvey Cushing was the first to advocate early and definitive debridement of necrotic tissue, removal of all in-driven debris and meticulous dural and scalp closure. He could reduce the operative mortality from 54% to 28%.1 During the early part of World War II and the Korean war, brain abscesses were routinely found in association with retained bone fragments.2-4 Because of this experience aggressive initial debridement of the missile tract was adopted during the Vietnam war and as a result the infection rate declined from 53% to 15% and surgical mortality was also markedly reduced.5 Despite these results the issue of the causal relation of retained bone fragments with the development of brain abscess remained speculative as there was evidence to the contrary as well. Maltby6 found only 3 cases of retained bone fragment in a group of 17 cases of brain abscess during World War II. Experimental studies by Pitlyk et al7 also noted only 4-8 % incidence with sterile and contaminated bone fragments if not combined with hair or scalp. Studies from Vietnam did not find any evidence to incriminate retained bone fragment in the development of brain abscess.8,9 With the availability of computerized tomography (CT scan), rapid evacuation of casualties, and better follow-up neurosurgical care, a less aggressive intracranial debridement with emphasis to preserve the brain tissue was adopted during the Israeli- Lebanese and Croatian conflicts and the outcome was better.10,11 Though great attention has been paid to brain injury, dural repair and scalp closure, the treatment of fractured bone has been neglected. Bone was discarded either after block resection1 or after craniectomy as advocated by Matson.12 This has been the general practice till the recent past,10 though early attempts to preserve the bone have also been made.2,13 We are presenting our experience of 60 cases of missile injuries treated with less aggressive debridement of missile tract, preferring craniotomy over craniectomy whereever feasible and in case of craniectomy, bone fragments were replaced if the condition of the brain and the wound permitted, thus avoiding future cranioplasty. MATERIAL AND METHODS During a period of one year from January 1999 to December 1999, 60 cases of missile injuries of the brain were treated at our hospital. Twenty-two of these cases were involved in the Kargil war and 38 in other militancy related activities in the state of Jammu and Kashmir. Thirty cases were directly evacuated to our hospital and 30 cases came after initial treatment at other forward hospitals.8 Of these 8 were operated and the remaining 22 were not operated on, but administered antibiotics and applied sterile dressings. The average time of arrival at our hospital was 30 hours but varied from 4 to 120 hours. All patients were assessed for patency of airway, breathing pattern and circulatory status. Neurological assessment was done by the Glasgow coma scale [GCS] score, pupillary size and reaction, other brainstem reflexes and limb movements. Local examination of the missile wound and examination of other systems was carried out elaborately. Resuscitative measures were initiated if the patient required respiratory support or was hemodynamically unstable. Patients having a GCS score of less than 8 were intubated and ventilated. X-ray skull was done in all cases and CT scan was done in 54 cases. Magnetic resonance imaging [MRI] study was done in 5 cases. Wound cultures were done in 20 cases. All patients were put on sodium penicillin, gentamicin and cefotaxime. Metronidazole was added if the missile had traversed any air sinus. Parenteral phenytoin and ranitidine were also started. Mannitol and lasix were given if features of raised intracranial pressure were seen on imaging studies. Fifty-two patients were operated at our center; of which 46 were initial debridement cases and 6 were re-operations after initial debridement at forward hospitals. The operative procedure comprised debridement of the scalp wound and then "Z" or "S" extension of this wound or raising of scalp flap depending upon the requirement of the skull exposure or closure of scalp wound. A craniotomy was performed centered over the skull penetrance. The margins of the missile tract in the bone were minimally (0.5 to 1cm) debrided. The size of the craniotomy was dictated by underlying brain damage. A craniectomy was performed if there was extensive comminution of the skull bone or if the wound was badly contaminated. The dural wound was completely exposed and its shredded margins trimmed and then the dural opening enlarged with further extensions as required. Superficial necrotic brain tissue was removed with suction and the missile tract was washed with saline using a catheter. No suction was introduced into the missile tract. Missile or bone fragments that presented themselves into the wound were picked up with forceps and removed. No extra maneuver was made to remove all the missile and bone fragments seen on the imaging studies. Hemostasis was achieved with bipolar coagulation and no gel foam or surgicel was used for achieving hemostasis expect for venous sinus injuries. The missile tract was finally washed with hydrogen peroxide and saline. The dural defect was repaired with a pericranial or temporal fascia to achieve a watertight closure. The bone flap was replaced and fixed with vicryl sutures. In case of craniectomy large bone fragments were washed with saline and replaced back. The wound was now irrigated with 1% povidone iodine. The scalp was closed in double or single layer with a subgaleal drain. Postoperatively antibiotics continued during for 2 weeks and anti-epileptics continued even thereafter. Cerebral decongestants (mannitol, frusemide and glycerol) were continued as dictated by the extent of the injury and if required postoperative ventilation was instituted. ICP was monitored for 72 hours in 10 patients who had a poor GCS score and extensive brain injury. All the 55 surviving patients were followed up to 6 months after injury. Complete neurological assessment, X-ray skull and CT scans of the head were done in all cases. RESULTS A total of 60 patients with missile injuries of the head were admitted to the Command Hospital (NC) C/O 56 APO. Their ages ranged from 19 to 40 years with a mean age of 25 years. There were 59 males and 1 female. Forty-three injuries were caused by shrapnel of shells, 12 were gunshot wounds and 5 by indigenous explosive devices (IEDs). The regional distribution is given in Table 1, parietal being the most common followed by the orbito-cranial /facio-cranial penetration. Punctate wounds were found in 10 cases and the remaining 50 had significant scalp laceration and brain matter was herniating out in 40 of these. The GCS score was 3-5 in 8, 5-8 in 14, 8-12 in 30 and 13-15 in 8. Associated eye injuries were found in 7, facial in 8, limb in 10, chest in 3 and tracheal injuries in 1 patient. X-ray skull was done in all cases and revealed skull penetrance without significant comminution in 35, in 10 cases extensive comminution of bone was found, and missile fragments were seen in 48 cases. CT scan of the head was done in 54 cases and was helpful in assessing the extent of brain damage and the location of bone and missile fragments. Details of CT scan findings are given in Table 2. In 15 patients CT scan revealed small hemorrhagic contusion with in-driven bones without significant mass effect, contusion with mass effect was found in 36 cases, cortical contusion without in-driven bones in 3, distant intracranial contusion in 4, intraventricular hemorrhage in 5, and multilobar injury in 14 cases. Missiles fragments were found at the distal end of the injury tract and bones at the proximal. MRI study was done in 5 cases in whom the missile had passed through the skull and X-ray did not show any missile fragments in the head or any other part of the body. Though the missile tract and brain contusion could be appreciated, bone fragments could not be appreciated on the MRI scan, however, brainstem contusion away from the missile tract was seen in 1 case. Acute surgeries were performed in 52 patients of whom 6 were re-operations for inadequate initial surgery done at forward hospitals. The time interval between the time of injury and the time of surgery varied from 6 to 72 hours with an average of 36 hours, however, antibiotics were started within 6 hours of injury in all patients. 30 cases were operated within 24 hours of injury, 10 between 24 to 48 hours and 12 were operated between 48 to 72 hours after injury. This delay was due to the delay in the evacuation from forward hospitals. In 3 cases of punctate wounds, and 3 cases of orbito-cranial injuries no surgery was done as they had minimal intracranial injury and had reached our center 96 hours after the injury. Two patients were treated with simple wound closure at forward hospitals within 24 hours of injury. For exposure of the skull, the scalp flap was raised in 20 cases and in 32 cases the missile wound was extended with `Z' or `S' extension. Craniotomy was done in 42, of which 18 were frontal, 19 parietal, 3 temporal, and 2 occipital. Craniectomy was done in 10 cases and in 7 of these bone fragments were replaced back. In the remaining 3 the bone was discarded due to an unhealthy looking wound in 2, and a swollen brain in 1 case. All but 2 wounds healed primarily, 2 patients developed mild scalp wound sepsis, (craniectomy + bone replacement group). Three others developed aspiration pneumonia; septicemia and lower limb deep vein thrombosis developed in 1 each. One patient developed posttraumatic hydrocephalus. There was no case of CSF leak in operated cases. Two of the three cases of orbito-cranial injuries treated conservatively, developed CSF orbitorrhoea and were subsequently operated. Five patients in our series died in the postoperative period, within a week of surgery. Three of these had a GCS score of < 5 and 2 had a score of <8. Other factors in these cases are depicted in Table 3. Our follow-up period varied from 3 to 9 months with an average of 6 months. The outcome as per the Glasgow scale was good in 42, moderate disability in 7, severe disability in 6 and death in 5 cases. The disabling factors were aphasia in 1, hemiplegia in 4 and significant cognitive function impairment in 1 case. There was no case of brain abscess formation or osteomyelitis of craniotomy bone flap or replaced bone fragments. However 20, (36.3%) of our cases revealed retained bone fragments and 18 (32.7%) revealed missile fragments on follow-up CT scans. DISCUSSION Till the availability of the CT scan, the dictum in the management of missile injuries of the brain had been to aggressively debride the missile tract, with an effort to locate and remove all the in-driven bone and metal fragments, even to the extent that re-operation was strongly recommended if postoperative radiographs showed residual bone fragments.3,5 Studies from Vietnam showed that only a small percentage of brain abscesses were associated with bone fragments and despite aggressive debridement 23% cases were found to have residual bone fragments on CT scan study. Therefore, re-operations on asymptomatic patients are not warranted.8,9,14 With the availability of CT scan a less aggressive surgical approach has been used successfully by many neurosurgeons in civilian and military missile injuries of the brain.10,11,15 CT scan is essential for such an approach to obviate the need for extensive exploration and to limit the surgery, for decontamination of the wound, hemostasis and to reduce intracranial pressure. Our results confirm that a less aggressive approach gives equally good results in these cases. Though the surgical mortality rate reported in the aggressive debridement group was lower than the less aggressive group,10,11 the studies are not matched. Higher mortality in the less aggressive groups has been attributed to more serious patients in in this group in these series. 10,11 Our mortality rate of 8.5% favorably matches 11% surgical mortality reported in more aggressive debridement, 16 despite the fact that even patients with a GCS score of < 5 were operated. The point whether one should operate on a patient with a GCS of < 5 or not, remains debatable. Though Grahm et al17 advocate no surgery for this group of patients if they have no intracranial mass lesion, we in our series found intracranial mass lesion in all patients in this category. Five out of 8 patients with a GCS of < 5 in our series survived, 3 with severe disability and 2 with moderate disability. Therefore, to withhold surgery in this group of patients may be rather difficult, even though the result of surgery may be poor. One of our patients in whom the missile had passed through the skull and in whom MRI could be done, had evidence of distant effects of missile injury on the brainstem along with large contusion of temporal lobe; he died despite surgery. Although, no definite conclusion can be drawn on the basis of 1 case, it appears that when brainstem injury is demonstrated on imaging, there is no benefit in operating on such a patient even in the presence of mass lesion. The GCS score has been found to be the main determinant of the outcome in our series (Table 3). A lower GCS score predicts poor outcome and a higher one a better outcome.10,15,17 Other factors, which are associated with a poor outcome, are multilobar injuries, intraventricular hemorrhage and dominant hemispheric injuries, as is evident from Table 2. Similar observations have been made in earlier studies.10,11,15,17 One of the main concerns of less aggressive surgery has been the fear of the development of brain abscess. 3,5,8 However, studies from the Vietnam war, reported an incidence of 8.4% 8 when a more aggressive surgical approach was adopted, and an incidence of 1.8 to 10%10,11 in a less aggressive approach. Various factors associated with the development of intracranial sepsis in missile injuries of the brain are CSF leaks, skull base injuries, extensive brain injury, prolonged coma, transportation time of > 48 hours and retained intracranial missile and bone fragments.3,8,19 In the absence of other factors brain abscesses do not occur in patients with retained bone or missile fragments.8,9 In our series we had no case of brain abscess. Though our period of follow-up is comparatively shorter than the other series,8,10,11 since the majority (90%) of brain abscesses develop within 6 weeks of injury,20 the chances of late abscess formation will be remote. The main factor, which may relate to such a result in our series, is that we had no CSF leakage from operative wounds and the majority (40 at our center and 8 at forward hospitals) of our cases were operated within 48 hours; and maybe early institution of effective antibiotics against intracranial infections at forward hospitals might have contributed to some extent towards this result. Various regimes of antibiotics from only methicillin to a combination of penicillin, chloramphenicol, aminoglycosides and metronidazole have been used with a reported intracranial infection incidence of 5-10%.11,21 We have used a combination of penicillin, aminoglycoside and 3rd generation cephalosporin, metronidazole was added if an air sinus was transgressed and there was no perioperative intracranial sepsis. We had 2 cases of wound sepsis which could be managed without surgery. During the 6 months review, CT scan did not show any evidence of intracranial sepsis. Whether early institution of antibiotics at forward hospitals or the use of our combination of antibiotics helped towards this result, is difficult to say. However, it appears that antibiotics are no substitute for early surgical debridement. 36.3% of our cases had retained bone fragments and 32.7% missile fragments and none were associated with brain abscess, thereby supporting earlier observations that retained bone and missile fragments are usually not the cause for the development of brain abscesses.8-11,21 The indications for craniectomy and craniotomy have not really been outlined. Cushing was the first to advocate and practice en-block resection of cranial bone in missile injuries of the brain during World War I and centrifugal craniectomy was a routine procedure during World War II and thereafter,10,12 even though there have been attempts to preserve the bone as well. Ascroft could preserve the vascularized bone fragments2 and Cairns advocated craniotomy for a small clean wound.3 The criteria for the selection of craniotomy and craniectomy were laid down by Rich et al22 i.e. if the exposure required is large, the surgery is done shortly after the injury is sustained, and if there is no gross contamination of the wound and no significant comminution of bone. We have only considered gross contamination of the wound, extensive comminution of bone and rarely, brain swelling, and could perform craniotomy in 42 cases even when surgery was done up to 72 hours after injury and had no postoperative osteomyelitis or wound sepsis. Whereas 2 patients in the craniectomy group developed wound sepsis none developed osteomyelitis. It appears that if the wound is not badly contaminated these skulls can be reconstructed with mini or microplates wherever available, thus avoiding subsequent cranioplasties. Our follow-up has been too short to comment on the chronic seizure disorder but an incidence of 22% in a 6-year follow-up in the less aggressive debridement group (10), and 29% in a 2-year follow-up in the aggressive debridement group (23) has been reported. A relatively low incidence in the less aggressive surgery group has been attributed to lesser cortical volume loss. REFERENCES 1. Cushing H. A study of series of wounds involving the brain and its enveloping structures. Br J Surg 1918;5:558-684.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03067t2.jpg] [ni03067t1.jpg] [ni03067t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}