 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
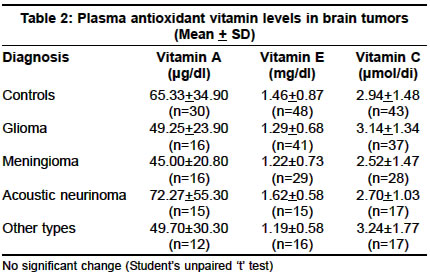
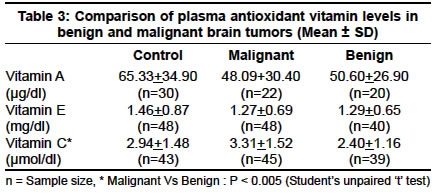
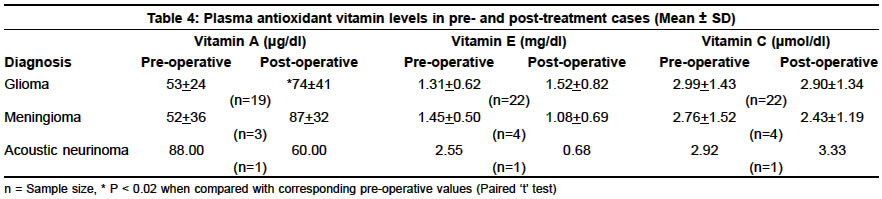
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 220-222 Plasma antioxidant vitamins in brain tumors G. M. Rao, A. V. Rao,* A. Raja,** S. Rao,** A. Rao*** Department of *Biochemistry, Kasturba Medical College, Mangalore and Department of **Neurological Sciences and Department of ***Biochemistry, Kasturba Medical College and Hospital, Manipal-576104, Karnataka, India. A. Rao Accepted on 20.08.2001. Code Number: ni03068 ABSTRACT Plasma levels of vitamins A, E and C were analyzed in 102 patients with different types of brain tumors. A follow-up study was done with 27 postoperative patients. On comparison with plasma from normal individuals, vitamin A and E were decreased, but the decrease was statistically insignificant. Vitamin C levels remained in the normal range. In a comparative study of preoperative and postoperative cases, plasma vitamin A levels in postoperative glioma patients were significantly higher than those in the pre-operative state. There was no significant difference in the plasma level of vitamins C and E. The results of the present study suggest that the plasma antioxidant vitamins are not altered effectively in brain tumor cases. Key Words: Vitamin A, Vitamin E, Vitamin C, Brain tumors. There is growing evidence implicating free radicals in a wide variety of medical diseases and conditions such as cancer and cardiovascular diseases. Epidemiological findings and animal studies support the belief that vitamins protect against cardiovascular diseases and probably cancer.1 Vitamin A and carotenoids have been considered antioxidants because of their capacity to relieve oxidative stress.2,3 They prevent lipid peroxidation by scavenging free radicals and other reactive oxygen species.4 Moreover, the vitamin has been implicated as a biological factor in reducing the incidence of cancer.5 Vitamin E is a lipid soluble chain breaking antioxidant.6 It may have an implication in the prevention of Alzheimer's disease, coronary heart disease and pretreatment may be a valuable method for myocardial protection.7,8 Pre-treatment of animals with α-tocopherol has been reported to lessen secondary damage in several models of ischemic or traumatic injury to CNS.9,10 An increase in vitamin E is observed in esophageal cancer.11 Several studies found lower plasma vitamin E in patients with existing lung cancer and oral cancer.12-14 Ascorbate reacts rapidly with superoxide and peroxyl radicals and even more rapidly with hydroxyl radicals to give semidehydroascorbate. Ascorbate can diminish the carcinogenicity of nitrosocompounds by reducing the nitroso group to an inactive product or by diminution of endogenous fecal mutagens.15,16 It has been established that a significantly increased relative risk of gastrointestinal cancer exists at low concentration of vitamin C.17-19 Furthermore, deficiency of vitamin C causes oxidative DNA damage and impaired immune response.15,16,20 There are no reports on plasma levels of vitamins A and E, and very few on levels of vitamin C in patients with brain tumor. In the present study, an attempt has been made to assess the plasma antioxidant vitamin status in such patients and evaluate the possibility of their role in preventing oxidative damage. MATERIAL AND METHODS Plasma samples from 102 patients, aged between 40-80 years, with different types of brain tumors including glioma, meningioma, acoustic neurinoma and other types (secondary tumors, tuberculoma, lymphoma, ventricular tumor and craniopharyngioma, Table 1), were studied. Healthy subjects (n=47) matched for age and sex were also studied as a control group during this period. Postoperative blood samples were obtained from the patients when they were reexamined at a follow-up study. Blood was collected in EDTA bottles. It was immediately centrifuged under refrigeration at 3000g for 10 minutes. The plasma was carefully separated and the vitamins estimated immediately. The estimation of vitamin A was done by the method of Paterson and Wiggins.21 Vitamin E levels were determined by the method of Bieri et al.22 Vitamin C was estimated chemically by using dinitrophenylhy-drazine as a color compound.23 Statistical analysis was done according to Student's paired and unpaired `t' test. RESULTS The plasma vitamin A and vitamin E levels showed a tendency to decrease in most of the brain tumor patients except in acoustic neurinoma, where the mean values showed a tendency to increase. However, a statistically significant difference was not observed in any of the study groups, when compared with the control group. Vitamin C levels remained in the normal range (Table 2). A drop in the mean plasma vitamin A and tocopherol levels was observed in both, benign and malignant brain tumor patients when compared to controls but this was not statistically significant. Low levels of plasma ascorbate were observed in patients with benign lesions whereas those with malignant tumors showed an increase in the vitamin C levels when compared to the controls. The increase in plasma ascorbate levels in patients with malignant tumors was significant (p < 0.005) when compared to those with benign lesions (Table 3). In the follow-up study, plasma vitamin A levels in postoperative glioma patients were significantly higher (p < 0.02) than those in the preoperative state. There was no statistically significant difference in plasma vitamin E and vitamin C levels in a comparative study of preoperative and postoperative samples (Table 4). DISCUSSION Retinol has long been known to be an effective antioxidant because of its capacity to scavenge free radicals. By quenching free radicals it protects lipids against peroxidation. Comstoc et al24 observed low levels of retinol and β-carotene in patients with cancer. Stone and Troll25 reported that retinol and its analogues, retinyl acetate and retinoic acids are effective inhibitors of superoxide radical production in polymorphonuclear leukocytes. A high serum vitamin A concentration has been reported to have a beneficial effect on the outcome of ischemic stroke.26 It has been established that there is a significantly increased relative risk of gastrointestinal cancer at low levels of vitamin A.27 This report is similar to the findings in the present study of low levels of plasma vitamin A in most brain tumors. Vitamin A deficiency is well known to result in metaplasia and facilitation of tumors in experimental animals. In humans, vitamin A and β-carotene reverse precancerous leukoplakia and reduce the occurrence of pathological micronuclei even on continuous exposure to mutagens from betel-nuts and tobacco chewing.28 Faber et al,29 in their preliminary study, reported that the plasma vitamin A level was not modified either in patients with cancer or after chemotherapy. Numerous studies have evaluated the neuroprotective efficiency of pharmacological agents with lipid antioxidant activity in models of spinal cord and brain injury. A decrease in lipid peroxidation and an increase in the activity of antioxidant enzymes have been observed after the administration of α-tocopherol and Se during the treatment of brain impairment.9 Intensive pretreatment of animals with endogenous lipid peroxyl radical scavenger, α-tocopherol, with 21-aminosteroids has been shown to decrease post-traumatic spinal ischemia and enhance chronic neurological recovery.9,10 Low levels of plasma vitamin E levels, as shown in our study, may facilitate oxidative damage in these patients. A protective effect on lipid peroxidation of vitamin C has been well established by Simon30 and Matsuda et al.31 Vitamin C may help to reduce the free radical damage and atheroma formation in blood vessels.32 Significantly reduced vitamin C levels have been reported in astrocytomas.33 The plasma vitamin C levels in cases of brain tumor in this study were within normal limits. Moreover, the marked increase in vitamin C levels in malignant cases over those observed in benign tumors may be due to the fact that more of ascorbic acid is used to regenerate vitamin E in membranes in these cases.34 The patients and controls in this study belonged to a homogeneous population with no differences in their cultural or socio-economic status. Hence, nutritional differences between the two groups are minimal. Therefore, the results of the present study suggest that the plasma antioxidant vitamins are not affected much in brain tumors. However, this does not overrule any possibility of alteration of vitamins at the site of the tumor. Further, the decreased activity of antioxidant enzymes35 accompanied with increased lipid peroxidation36 may be the major factors responsible for the oxidative stress observed in these cases. REFERENCES 1. Packer L. Protective role of vitamin E in biological systems. Am J Clin Nutr 1991;53:1050s-55s.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03068t2.jpg] [ni03068t3.jpg] [ni03068t4.jpg] [ni03068t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}