 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 237-240 Association of primary central nervous system lymphomas with the Epstein-Barr virus C. R. Rao, K. Jain, K. Bhatia,* K. C. Laksmaiah, S. K. Shankar** Kidwai Memorial Institute of Oncology, **Department of Neuropathology, NIMHANS, Bangalore, India; and *King Fahad National Centre for Children's Cancer and Research, Kingdom of Saudi Arabia. S. K. Shankar
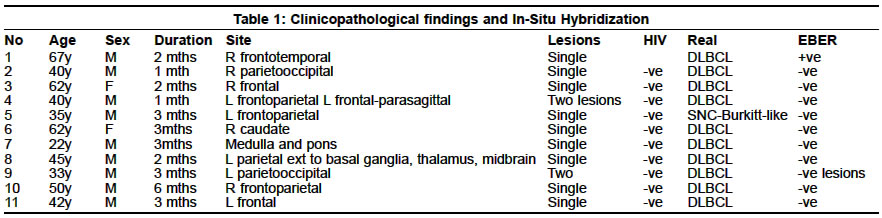
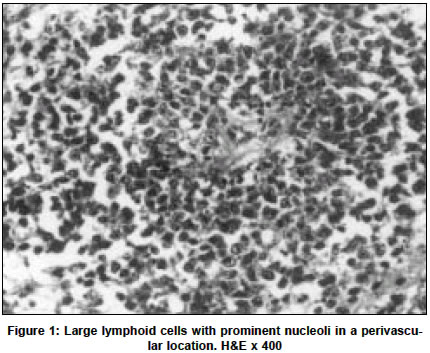
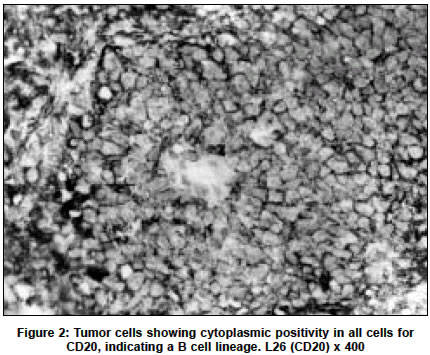
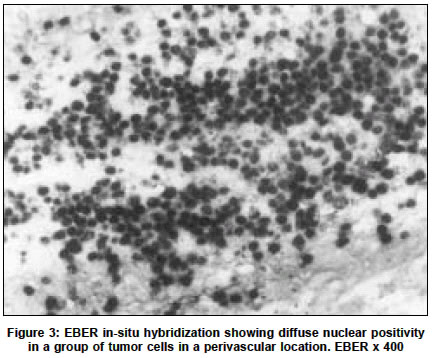
Accepted on 21.05.2001. Code Number: ni03072 ABSTRACT The incidence of primary central nervous system lymphoma (PCNSL), previously a rare tumor, has increased significantly over the past few decades, partly due to the AIDS epidemic but also in immunocompetent individuals. Studies from Western countries have shown a consistent association of tumors occurring in immunocompromised individuals with the Epstein-Barr virus (EBV) suggesting an important role for the virus in the pathogenesis of these tumors, but an infrequent association of the virus with PCNSL in the immunocompetent host has also been noted. We studied 11 patients with PCNSL who had no evidence of an immunocompromised state. All the tumors were aggressive B cell lymphomas. EBV association was studied using EBER in-situ hybridization. 10 out of the 11 tumors were negative for EBV, indicating that tumors in immunocompetent individuals in developing countries are also infrequently EBV associated and that a different pathogenetic mechanism is operative in the evolution of these tumors. Key Words: Epstein-Barr virus, Primary CNS lymphomas, Immunocompetent individuals. Primary central nervous system lymphoma (PCNSL) is an extranodal aggressive nonHodgkin's lymphoma, which arises in and is confined to the central nervous system in the absence of systemic malignancy, although extracerebral spread may occur in the later stages of the disease.1,2 These are rare tumors which until recently constituted less than 1% of all primary cerebral tumors and 0.5-2% of all non-Hodgkin's lymphomas.2,3 Reports from industrialized countries over the last two decades, including reports from the National Cancer Institute SEER Program, have shown a more than tenfold increase in the incidence of PCNSL, which is partly associated with the AIDS epidemic, but which has also occurred in immunocompetent individuals.4,5 This striking increase in incidence resulted in PCNSL being referred to as the `new epidemic'.6 However, brain lymphomas were not projected to surpass glial tumors as the most frequently diagnosed intracranial malignancy by the year 2000.5 The association of EBV with PCNSL in AIDS patients is 75-100% in different series, indicating an important pathogenetic role for the virus in these patients. PCNSL occurring in immunocompetent individuals is, however, infrequently associated with the virus, suggesting that a different pathogenetic mechanism is operative in these cases.7-19 We have investigated the association of PCNSL occurring in immunocompetent individuals, with EBV in southern India. A significant association of EBV with other tumors like Burkitt's lymphoma (80%) and Hodgkin's disease (78%) has been documented from oncology centers in India,20-22 similar to the findings from other developing countries.23-25 There is no data from the developing countries on the association of EBV in immunocompetent individuals with PCNSL. This brief communication addresses this issue based on a limited sample sourced from one center. MATERIAL AND METHODS Case Selection: Eleven cases of PCNSL diagnosed between 1989 and 1996 were accessioned from the pathology files of the Kidwai Memorial Institute of Oncology in Bangalore, India. All the patients were referred after a biopsy/surgery at the National Institute of Mental Health and Neurosciences, Bangalore. Only those cases were included in the study in which the initial presenting symptoms and signs were referable to the central nervous system and, there was no peripheral lymphadenopathy, organomegaly or evidence of bone marrow involvement at presentation. There was no history or clinical findings to suggest an immunocompromised state. Ten patients were HIV negative. The HIV status was unknown but considered negative based on the clinical criteria. Histopathology, including immunophenotyping In-situ hybridization RESULTS (Table 1) Clinical findings: The age of the patients ranged from 21 to 67 years, with a mean of 45 years and a median age of 42 years. The male to female ratio was 4.5:1. The duration of symptoms varied from 1 month to 6 months, 10 out of 11 patients presented with symptoms of 3 months' duration or less. The tumors were supratentorial in 10 cases, the frontal and parietal regions being the sites most commonly involved. The brainstem was involved in 1 case. The tumors were multiple in 2 cases. The right and left sides of the cerebrum were involved with equal frequency. Histopathology/Immunophenotyping: Ten out of eleven cases were diffuse large B cell lymphomas (Figure 1). One case was Burkitt-like in morphology. All cases showed cytoplasmic positivity of all cells with CD20 (Figure 2), indicating that they were of B cell origin. CD3/UCHL-1, both markers for T cells, were negative in the tumor cells. Insitu hybridization for EBV: ISH for EBV was negative in 10 out of 11 cases. One case, which was histologically a diffuse large B cell lymphoma in a 67-year-old male, showed focal positivity for EBV. Positivity was indicated by strong diffuse nuclear staining. The positive cells were groups of tumor cells in a perivascular location (Figure 3) and individual cells scattered randomly through the tumor. Other cells in the vicinity like the endothelial and smooth muscle cells of the blood vessels, and glial and neuronal cells were negative. This patient was diagnosed in 1989 and his HIV status was unknown, though clinically not suggestive. U6 was positive in all cases indicating adequate RNA preservation. DISCUSSION The incidence of PCNSL has increased significantly over the past two decades, the increase being much more than that of NHL (Non- Hodgkin's Lymphoma) in totality.5 This increased incidence is partly associated with the AIDS epidemic, but has also occurred in immunocompetent individuals.4,5 Symptomatology is usually of short duration (one to two months) and the peak incidence is in the fifth to seventh decades; AIDS-associated PCNSL occurs in a younger age group (in the third to fourth decade).2,3 Interestingly, although there was no evidence of any pre-existing immunocompromised state, five of our patients were 40 years of age or younger. The most common histological subtypes encountered among PCNSL, in both immunocompromised and immunocompetent individuals, are the aggressive B cell lymphomas, diffuse large B cell lymphoma being the most frequent (>50%), followed by small non-cleaved cell lymphomas. Low-grade B cell and T cell lymphomas are rare (12%).2,3,27,28 All our cases, except for one, were diffuse large B cell lymphomas. The association of EBV with AIDS-related PCNSL varies from 75%-100% in different series. PCNSL occurring in immunocompetent individuals is, however, infrequently associated with the virus.7-19 From developing countries there are no reports of the association of PCNSL with EBV in immunocompetent individuals. Investigating this association would be especially interesting because reports from developing countries, including our data, have shown a high prevalence of EBV in other lymphomas like Burkitt's lymphoma and Hodgkin's disease.20-25 However, only one patient in this preliminary series of PCNSL was EBV positive. Although the HIV status of this patient was unknown, he had no other symptoms or clinical findings to suggest an immunocompromised state. EBV positivity in this case was also only focally identified (<10% of cells) which resembles the pattern of positivity reported in immunocompetent individuals where only a small proportion of tumor cells exhibit the virus in contrast to AIDS-PCNSL where the majority of cells are EBV positive.12,17 PCNSL occurring in immunocompetent individuals is, therefore, possibly a different pathological entity, resembling systemic Diffuse Large B-Cell Lymphoma which is also infrequently EBVassociated,29,33 thus indicating that EBV may not be involved in the pathogenesis of these two entities. Demonstration of the virus in only a subpopulation of tumor cells also raises the possibility of secondary EBV infection of tumor cells, although loss/shedding of viral genomes from the tumor cells of an EBV positive neoplasm is also a possibility.29 Unlike Burkitt's lymphoma and Hodgkin's disease, where the prevalence of EBV in the tumor varies depending on geographic location,23,34 this study from a developing country, although the numbers are small, suggests that the lack of a significant EBV association with PCNSL in immunocompetent individuals is universal. Further studies on a larger number of patients from different geographic areas would be essential to resolve this issue of the oncogenic association of the virus. REFERENCES 1. Hochberg FH, Miller DC. Primary central system lymphoma. J Neurosurg 1988;68:835-53.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03072f1.jpg] [ni03072f2.jpg] [ni03072t1.jpg] [ni03072f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}