 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 246-247 Case Report Cerebellar hemisphere, an uncommon location for pleomorphic xanthoastrocytoma and lipidized glioblastoma multiformis S. Kumar, T. M. Retnam, G. Menon, S. Nair, R. N. Bhattacharya, V. V. Radhakrishnan* Department of Neurosurgery, *Neuropathology, Sree Chitra Tirunal Institute for Medical Sciences & Technology, Thiruvananthapurum-695011, India. V. V. Radhakrishnan
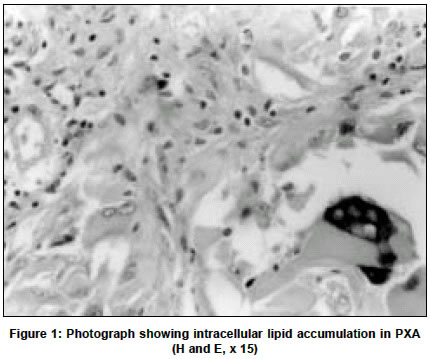
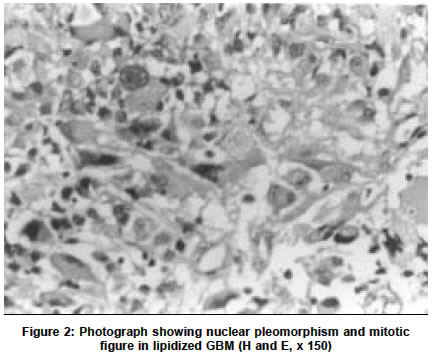
Accepted on 27.06.2002. Code Number: ni03075 ABSTRACT Lipidized glioblastoma multiformis (LGB) and pleomorphic xanthoastrocytoma (PXA) are often supratentorial in location and occur in the second to fourth decade. This report presents two young patients, one having LGB and the other having PXA in the cerebellum. Histological differentiation between LGB and PXA is discussed. Key Words: Lipidized glioblastoma multiformis, pleomorphic xanthoastrocytoma Lipidized glioblastoma multiformis (LGB) and pleomorphic xanthoastrocytoma (PXA) are two distinct clinicopatbological entities. Both the tumors occur in the second to fourth decade and are often supratentorial in location. Cerebellar location is extremely uncommon. This report describes the characteristic histopathological features and emphasizes the distinguishing histopathological features between PXA and LGB. CASE REPORT Case 1 A 15-year-old male was admitted with history of headache and vomiting of one-month duration. Other than papilloedema, there was no neurological deficit. Investigations revealed a right cerebellar solid mass with cystic degeneration. There was obstructive hydrocephalus. Right retro-mastoid craniectomy and subtotal resection of the tumor was done. The tumor was moderately vascular and the cyst contained xanthochromic fluid. Histological examination showed an admixture of spindle cells and mono- or multi-nucleated giant cells. Neoplastic cells had nucleoli of variable size and shape, some of the cells showed characteristic intracellular accumulation of lipid vesicles (Figure 1). Eosinophilic granular bodies were also seen in between the neoplastic cells. Characteristic xanthomatous cells surrounded by basement membrane were stained positive for reticulin. There was no necrosis, microvascular proliferation, or mitotic figures. Glial fibrillary acidic protein (GFAP) immunostaining showed varying degree of immunoreactivity in the neoplastic cells. Based on these histopathological features a diagnosis of PXA was made. Case 2 A 12-year-old child was admitted with a history of headache, vomiting and ataxia for two weeks. Neurological examination revealed papilloedema and left cerebellar signs. MRI showed a hypointense mass lesion having areas of necrosis with surrounding edema in the left cerebellar hemisphere. The patient underwent midline sub-occipital craniectomy and partial resection of the tumor. The tumor was moderately vascular with areas of necrosis and hemorrhage. Leptomeninges over the tumor were thickened and vascular. Hematoxylin and eosin-stained sections showed a cellular tumor with striking nuclear pleomorphism. The cell nuclei showed variation in size and shape (Figure 2). The lesion also showed an admixture of spindle cells, multi-nucleated giant cells, as well as lipidized and non-lipidized neoplastic cells. However, the most characteristic features were satellite necrosis, pseudo-palisading and numerous mitotic figures. Microvascular proliferation was also present. Neoplastic cells showed varying degree of immunoreactivity for GFAP. The reticulin stain showed deposition of reticulin fiber in the peri-advential region of the blood vessels. Based on histopathology features a diagnosis of lipidized GBM was made. DISCUSSION Pleomorphic xanthoastrocytoma (PXA) was recognized as a distinctive astrocytic tumor in 1979.1 The vast majority of PXA, occur in a supratentorial location with a striking predilection for the temporal lobe. Location outside the supratentorial compartment is extremely uncommon. Only five patients with cerebellar location have been reported.2-6 Often the tumor occurs in the second and third decade and the typical clinical presentation is with protracted seizures. Histological characteristics include marked cellular pleomorphism, multi-nucleated cells with bizarre hyperchromatic nuclei and fusiform cells. However, the most characteristic feature is the presence of intracellular multi-lobulated lipid vesicles. The amount of lipidized cells is variable. Other features include lymphocytic perivascular cuffing, granular eosinophilic droplets and reticulin-rich stroma. Mitotic figures and necrosis are usually absent. PXA is generally regarded as a lower grade tumor7 and following surgery the prognosis is generally good with good functional outcome.8 However, recurrence and malignant transformation have also been reported.9,10 Glioblastoma multiforme is the most common supratentorial malignant astrocytic tumor in adults. The cerebellum is an uncommon location. The salient histopathological features include cellular pleomorphism, nuclear atypia, brisk mitotic activity, multi-nucleated cells, microvascular proliferation and necrosis. Occasional lipidization of the neoplastic cells in glioblastoma has been reported.11,12 These features may be mistaken for PXA when lipidization is extensive and the location of the tumor is superficial, more so if the patient is young. The salient distinguishing features that differentiate LGB from PXA are: a) presence of brisk mitotic activity; b) necrosis; c) absence of characteristic reticulin-rich stroma in and around tumor cells. Malignant changes including mitotic figures and necrosis occur in recurrent PXA and may mimic an anaplastic astrocytoma or even a glioblastoma multiforme13 and a clear distinction may be difficult on histopathological grounds alone. REFERENCES 1. Kepes JJ, Rubinstein LJ, Eng LF. Pleomorphic xanthoastrocytoma: a distinctive meningocerebral glioma of young subjects with relative favorable prognosis. A study of 12 cases. Cancer 1979;44:1839-52.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03075f2.jpg] [ni03075f1.jpg] |
| |||||||||

{kind=link}
{kind=link}