 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
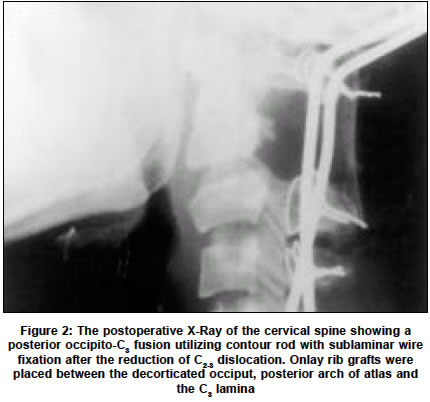
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 250-251 Case Report Congenital absence of the posterior elements of C2 vertebra: A case report P. Trivedi, K. H. Vyas, S. Behari Department of Neurosurgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Rae Bareli Road, Lucknow-226014, UP, India. Sanjay Behari Accepted on 26.03.2002. Code Number: ni03077 ABSTRACT A rare case of the complete absence of the posterior elements of C2 is reported. The patient presented with neck pain without any neurological deficits and radiology revealed a mobile, partially reducible dislocation of the C2 over C3 vertebra. A posterior fusion utilizing a contour rod, sublaminar wire fixation, and onlay bone grafts between the occiput and the C3 vertebra was performed for spinal stability. Key Words: C2 vertebra, Spinal dislocation, Spina bifida. The common developmental anomalies of the axis include anomalies of the odontoid process like total absence (agenesis); partial absence (hypoplasia); non-fusion of the odontoid process (os odontoideum); and segmentation failure of the second and third cervical vertebrae.1,2 Isolated anomalies of the posterior elements of the axis are extremely rare.3-9 We report a patient with complete absence of the posterior elements of the axis and spinal instability. CASE REPORT A 31-year-old woman was admitted with history of pain in the nape of the neck of two years duration. One-and-a-half months prior to the admission, there was an increase in the severity of the pain. She also felt stiffness while moving the head. There was no history of head or neck trauma. Her neurological examination did not reveal any neurologic deficits. Plain X-rays of cervical spine revealed complete absence of the pedicles, laminae and spinous process of the axis. There was partially reducible, mobile dislocation of C2 over C3 vertebra. The arch of atlas, the odontoid process and the cranio-vertebral junction were normal and there was no atlanto-axial dislocation (Figure 1). Magnetic resonance imaging (MRI) revealed obliteration of the anterior subarachnoid space against the C3 vertebral body but without any spinal cord compression. The dislocation reduced maximally on extension of the neck. The patient underwent a posterior occipito-C3 fusion utilizing contour rod with sublaminar wire fixation after the reduction of C2-3 dislocation. Onlay rib grafts were placed between the decorticated occiput, posterior arch of atlas and the C3 lamina. The postoperative X-Ray of the cervical spine (Figure 2) showed complete reduction of C2 over C3 vertebra. She was discharged with her neck movements stabilized using a hard cervical collar for three months. She had significant improvement in the neck pain. At one-and-a-half years follow-up she remained completely free of her neck symptoms. DISCUSSION Isolated anomalies of the posterior elements of the axis are extremely rare. Our review of the literature revealed only 4 reported cases of incomplete, congenital absence of the posterior elements of the axis and were described as spina bifida of C2 vertebra.3,6-8 The defect in these patients was in the spinous process and the lamina. Of the 4 patients, 2 presented with stenosis at C2 due to the invagination of the bifid lamina of C2 vertebra.3,6 Only 2 cases with complete absence of the posterior elements of the axis have been reported.9 The embryogenesis of this rare developmental anomaly is complex. The development of the vertebra occurs in three stages, which include precartilage, chondrification and ossification stages. In the precartilage stage cells of sclerotome migrate in three directions: ventromedially by surrounding the notochord, the cells form the vertebral body; dorsally they cover and form the neural arch; and ventrolaterally they form the costal process.3 Chondrification of the posterior arch begins at the pedicle during the sixth week of embryogenesis and ends in the midline during the fourth month. The cartilaginous arch ossifies by the age of 3 to 4 years.4 Thus the posterior element defect of the axis may be caused either by the failure of the extension of the chondrification centers in the posterior arch or by the failure of the ossification process. Complete absence of both the cartilaginous and bony components of the posterior elements implies a very early fault in embryogenesis.5 O'Rahilly and colleagues5 studied the cervical spine of nine embryos. According to them, at the stage of embryogenesis (eighth post-ovulatory week), the neural arches of the axis extend laterally from the centrum and also form a complete or incomplete foramen transversarium. During this period of embryogenesis, the neural arches proceed directly backward to a variable extent to form the pedicle, articular process and the lamina. A developmental defect during this stage or before could lead to the complete absence of the posterior elements. Surgical approach of spina bifida of C2 vertebra depended on the presenting clinical and radiological findings. In both the patients with stenosis at C2 due to the invagination of the bifid lamina of C2 vertebra, resection of the compressing bone resulted in the recovery of neurologic deficits.6 The patient in whom the anomaly was detected during radiographic study of the cervical spine was managed conservatively.7 The details of the fourth patient with spina bifida of C2 vertebra were not mentioned in the report.8 One of the patients with complete absence of the posterior elements of the axis had neurological deterioration following C1-3 posterior fusion.9 A subsequent transoral resection of the compressing segments of C2 and C3 bodies as well as the C2-3 intervertebral discs resulted in neurological improvement. With this experience by the authors, the second patient was operated first by the transoral route followed by C1-3 posterior fusion utilizing plates and sublaminar wires.9 In our patient, the C2-C3 dislocation was partially reducible and the patient did not have any neurologic deficits. A posterior fusion between the occiput-C3 vertebra using a contour rod, sublaminar wire fixation and onlay bone grafts supplemented the deficient middle and posterior columns of the axis that were responsible for the chronic instability. The good outcome in our patient makes us believe that the surgical approach which we adopted in our patient, is an appropriate option for this rare anomaly. REFERENCES 1. Gillman EL, Beach L. Congenital absence of adenoid process of axis: case report. J Bone Joint Surg Am 1959;41:345-8.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03077f1.jpg] [ni03077f2.jpg] |
| |||||||||

{kind=link}
{kind=link}