 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
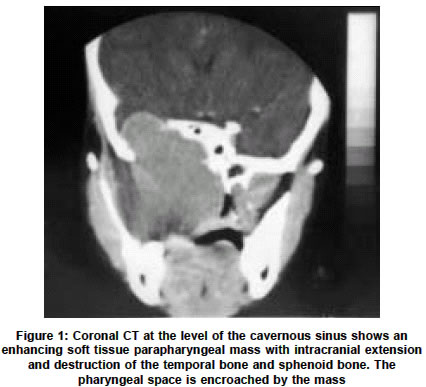
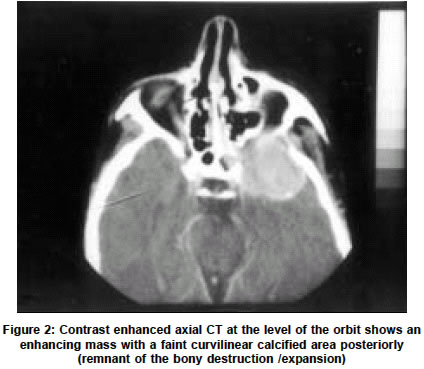
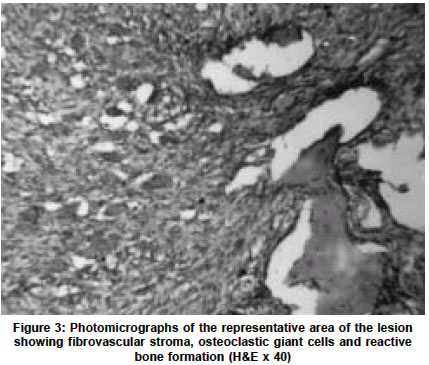
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 260-262 Case Report Giant cell reparative granuloma of the base of the skull presenting as a parapharyngeal mass S. Magu, S. K. Mathur,* S. P. Gulati,** A. Yadav, V. Kaushal*** Departments of Radiology, *Pathology, **Otolaryngology and ***Radiotherapy, Pt. B.D. Sharma PGIMS, Rohtak-124001, Haryana, India. Sarita Magu
Accepted on 27.10.2001. Code Number: ni03081 ABSTRACT Giant cell reparative granuloma is an infrequent non-tumoral lesion affecting the maxillary and mandibular bones and only rarely, the cranial bones. We report a case of giant cell reparative granuloma of the base of the skull in a 12-year-old female who presented with a parapharyngeal mass. Computerized Tomography (CT) showed the intracranial extension and destruction of surrounding bones. Key Words: Giant cell reparative granuloma, Giant cell tumor, Tumors of the skull. INTRODUCTION Jaffe coined the term `giant cell reparative granuloma' (GCRG) in 1953 to describe lesions of the maxilla and the mandible.1 There have been occasional reports of GCRG of the skull, especially involving the bones of the skull base. Similar tumors have been reported in the small bones of the hand and feet and long bones of the axial skeleton.2 Although regarded as a benign process, GCRG may be locally aggressive, and surgical excision is recommended wherever possible. We report a case of GCRG presenting as a parapharyngeal mass and having an intracranial extension. CASE REPORT A 12-year-old female presented with complaints of headache for 7 months. This was associated with right-sided facial swelling and episodes of epistaxis for the past 3 months. The swelling was tender on examination. Peroral examination revealed a swelling around the last upper molar tooth on the right side. As the patient had trismus, a thorough examination was not possible. Radiograph showed a soft tissue shadow in the region of the nasopharynx. CT at the level of the paranasal sinuses showed a homogeneous enhancing soft tissue mass in the right parapharyngeal region with associated destruction of the posterolateral wall of the right maxillary sinus eroding the base of the skull and extending intracranially into the region of the cavernous sinus (Figures 1 & 2). Laterally, the mass extended into the infratemporal fossa. Calcium phosphate, alkaline phosphatase, parathyroid hormone levels and urinalysis were normal. Fine needle aspiration smears from the swelling showed oval to spindle cells present in large and small groups and dispersed singly in a background of a large number of multinucleated giant cells, foamy macrophages, a few osteoblasts and RBCs. The cells showed moderate to abundant poorly defined cytoplasm with nuclei having fine reticulogranular chromatin and prominent nucleoli suggestive of giant cell lesion. Biopsy of the lesion showed benign osteoclastic giant cells scattered in a cellular fibroblastic stroma which was highly vascular (Figure 3). All these findings supported the diagnosis of GCRG and the patient was given radiotherapy as the tumor was inoperable. DISCUSSION The pathogenesis of GCRG was initially thought to be a hyperplastic reparative reaction to intraosseous hemorrhage induced by trauma.1 Other theories on the pathogenesis include infectious and developmental causes.4,5 There are two forms of GCRG, central arising from bone and peripheral arising from the soft tissues of the mandible or the maxilla. The preferred site is the facial bones. There have been sporadic reports of GCRG in other parts of the body. It is rare in the skull and has been found chiefly in the bones of the skull base: sphenoid, ethmoid and temporal bone.2 Chuong et al6 have outlined six criteria (pain, rate of growth, swelling, tooth root resorption, cortical perforation and recurrences) that may be used to classify the lesion as aggressive or non-aggressive. The symptoms vary according to the site of origin. The GCRG in our patient was quite large in size. Such large enhancing masses should undergo angiography to help pre-surgical planning. The differential diagnosis of GCRG includes aneurysmal bone cyst, benign chondroblastoma, the brown tumor of hyperparathyroidism, cherubism, fibrous dysplasia, non-osteogenic fibroma, osteosarcoma and true giant cell tumor (GCT).3 The hardest to distinguish from GCRG is the true GCT. In fact some believe that these lesions represent a continuum of the same disease process.7,8 Radiological examination rarely confirms the nature of the lesion. A differential diagnosis is to exclude other lytic and expansile lesions. On radiologic evaluation GCRG and GCT are indistinguishable. Both appear as non-specific lytic lesions of bone. Although usually solitary, these lesions can be multilocular. CT is excellent at detecting bony destruction and may represent the best tool for follow-up evaluation.9 In the case report of GCRG of the base of the skull by Cohen et al9 there was significant enhancement of mass after injection of intravenous contrast media as also observed in the present case. MRI is best used for evaluating the soft tissue structure surrounding the tumor. Both GCRG and GCT appear as low intensity signals on T1 and T2 weighted images which enhance slightly with Gadolinium contrast.10 Because of the non-specific nature of radiologic findings, histological evaluation and clinical behavior have been used in an attempt to distinguish GCRG from GCT.3 A GCT generally affects individuals between 25 and 40 years of age and very rarely under the age of 20. The stroma contains little or no intercellular material. Deposition of osteoid substance is rarely observed. The giant cells are uniformly scattered with a large quantity of nuclei and scanty cytoplasm. In GCRG the age at onset is usually younger (10 to 25 years), there are fewer giant cells with a smaller number of nuclei and a larger cytoplasmic component. Further, they are less uniformly distributed and are closely associated with microcystic or hemorrhagic zones.2 Differential diagnosis from brown tumors of hyperparathyroidism is based mainly on clinical and laboratory data such as serum and urinary levels of calcium, phosphates, nephrogenous CAMP, radioimmunoassay for parathyroid hormone, phosphate clearance, bone and serum alkaline phosphatase, and hydroxyprolinurea. One has to take into consideration the late onset and frequent multiplicity of the lesions. Aneurysmal cyst rarely poses problems of differentiation, especially if several zones of the sampled tissue, also involving the non-solid portion of the lesion, are studied.2 Treatment consists of curettage of the affected area, partial resection followed by low total dose of high-voltage radiotherapy. The main concern with radiation therapy is the potential for sarcomatous transformation.11 As the present case was not amenable to surgery, radiotherapy was instituted and long-term results of the same will have to be observed. Prior embolization to devascularize such masses is suggested to minimize preoperative bleeding. Such devascularized tumors also respond better to radiotherapy. It is important to recognize GCRG and differentiate it from GCT of bone, for while surgery or surgery plus radiotherapy often affords permanent cure from GCRG (only 12% to 16% of recurrences in large series) GCT calls for more aggressive treatment.2 GCT are associated with a higher incidence of recurrence (45-62%), metastasis (1-6%) and malignant transformation in contrast to low recurrence rates of GCRG (10-15%) and absence of metastasis.3 The histologic identification of the admixture of spindle cells, collagen, giant cells, and bony trabeculae are the most important features for the diagnosis of GCRG.12 There is an increased incidence of osteoid hemorrhage and hemosiderin in GCRG as compared with GCT. Other characteristics include fibrosis in GCRG, the absence of necrosis in GCRG, and a greater incidence of mitotic figures in GCT.3 GCRG affects females more often than males, mainly in the second and third decade.13 REFERENCES 1. Jaffe HL. Giant-cell reparative granuloma, traumatic bone cyst, and fibrous (fibroosseous) dysplasia of the jaw bones. Oral Surg 1953;6:159-75.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03081f1.jpg] [ni03081f3.jpg] [ni03081f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}