 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 266-268 Case Report Post-cardiorespiratory arrest beta-alpha coma: an unusual electroencephalographic phenomenon G. R. K. Sarma, A. Kumar, A. K. Roy, L. Pinheiro Department of Neurology, St. Johns Medical College Hospital, Bangalore, India. G. R. K. Sarma
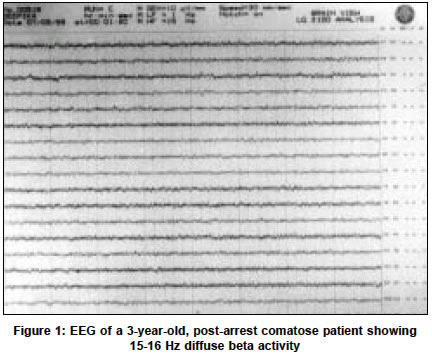
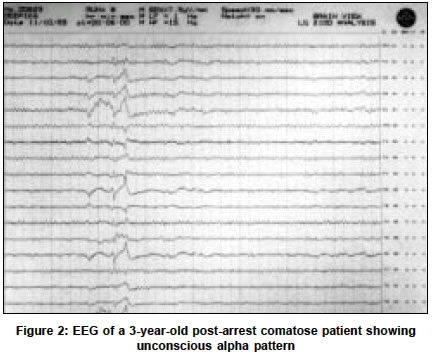
Accepted on 01.10.2001. Code Number: ni03083 ABSTRACT The presence of frontally-dominant alpha pattern in the EEG is common in patients with coma due to trauma, toxic-metabolic causes and following cardiorespiratory arrest. Diffuse beta activity following resuscitation after a cardiac arrest is not well recognized. We report a case of coma in a 3-year-old girl who had a cardiac arrest from which she was revived. Initial EEG showed diffuse beta activity, which later evolved to predominantly alpha activity. The possible mechanisms involved in the generation of such rhythms are discussed. Transition of EEG activity from faster to slower frequencies is suggested as an adverse prognostic factor in post-cardiorespiratory arrest coma. Key Words: Electroencephalogram, Cardiorespiratory arrest, Frontal brain. The presence of the frontally-dominant alpha pattern on the EEG is well recognized in coma from toxic and metabolic causes, and after resuscitation from prolonged cardiac arrest.1 Similarly, the presence of diffuse beta activity sometimes mixed with alpha activity is well known in drug- or anesthesia-induced comatose states.2 However, the presence of diffuse beta activity following resuscitation after prolonged cardiac arrest is not well recognized. Evolution of EEG patterns in comatose patients is also not systematically studied. The following report is of a patient whose post-arrest EEG showed diffuse beta activity which evolved into a predominantly alpha rhythm, which was unresponsive to any physiological maneuvers. CASE REPORT A 3-year-old girl underwent liver transplantation for treatment of congenital biliary atresia. Following surgery, she received cyclosporin (65 mg twice a day) and prednisolone (2.5 mg twice a day). Five months later, she developed headache, vomiting and an episode of generalized tonic-clonic seizures. This was followed by persistent drowsiness. Clinical examination did not reveal any neurological deficits. A clinical possibility of cyclosporin toxicity was considered. Serum levels of cyclosporin were in the toxic range (250 ng /ml). CT scan of the brain was normal. Biochemical investigations revealed hypernatremia, hypomagnesemia, metabolic acidosis and respiratory alkalosis. Cyclosporin was then discontinued. Phenytoin was administered and acidosis and hypomagnesemia were corrected. However, she suffered a prolonged cardiac arrest from which she was revived. She was hemodynamically stable following the resuscitation, but she had no spontaneous respiration, no response to deep painful stimuli, and no eye movements by oculo-cephalic maneuver. Pupils were dilated and non-reactive. Corneal and pharyngeal reflexes were absent. She was breathing with the help of a ventilator. Brainstem auditory evoked potentials were not recordable on 3 occasions. The ten-minute apnea test was negative. These tests suggested that she was brain-dead. However, in view of her young age (3 years) and the fact that the criteria for brain death are not specified in this age group, her life-support system was continued. She remained in this condition for 4 weeks. Tests for brainstem function including the apnea test remained negative. Life-support systems were maintained till she developed another cardiac arrest and died. A 16-channel EEG record was obtained at initial evaluation after connecting to the ventilator, using silver chloride disk electrodes placed at standard scalp sites according to the 10-20 international system with recording for 20 minutes. Intermittent photic stimulation was performed. The EEG revealed a mixture of predominantly 15-16 Hz diffuse beta activity (Figure 1) and scant, 8-9 Hz generalized alpha activity without responsiveness to passive eye opening. There were no epileptiform discharges. There was no response of the background activity to noxious stimuli or photic stimulation. A repeat EEG (Figure 2) obtained a month later showed a change in the background activity to a predominantly 8-9 Hz generalized alpha activity, which was poorly modulated, intermixed with scant 6-7 Hz theta activity. There was no posterior predominance of the alpha activity. No epileptiform discharges were noted. DISCUSSION In the present case, we noted an interesting pattern of initial beta, and later alpha activity after resuscitation from a prolonged cardiac arrest in a 3-year-old child. This pattern of serial change from beta to alpha pattern in post-cardiorespiratory arrest coma has not been described earlier. An alpha frequency in an unresponsive patient was first described by Loeb & Paggio in 19533 and was subsequently identified in four categories of patients including those following cardiorespiratory arrest, head trauma, those with brainstem lesions and toxic or metabolic abnormalities.4 More recent reports have extended the concept of alpha pattern coma to include theta frequencies (theta or alpha-theta coma).5 Kaplan in a meta-analysis of 36 patients with alpha pattern coma, found that 11 of these patients had concomitant beta activity.6 Only in 1 of these patients, beta activity constituted greater than 50% of the background activity. In contrast, Horton et al found that the EEG patterns of coma are more varied in children and may include alpha, beta, theta or spindle patterns.7 However, the outcome was not determined by the EEG patterns in their study. A number of conditions have been reported to cause beta activity in a comatose patient. These include barbiturate administration,8 benzodiazepines,9 clomethiazole,9 and severely disturbed glucose metabolism.10 However, our patient was not on any of these drugs and had no metabolic disturbance to account for the beta activity. Cyclosporin toxicity has been reported to cause temporo-occipital epileptiform discharges but excess beta activity has not been reported. Thus, it is most likely that the excess beta activity in our patient was due to the anoxic brain injury. The genesis of alpha frequency activity in comatose patients is incompletely understood. It is believed that the alpha frequency pattern in comatose patients represents a de novo rhythm sharing only frequency characteristics with the waking alpha rhythm. 11 Animal data suggest an analogy with the amygdaloid alpha spindle bursts in the 8-12 Hz range seen over the cerebral hemispheres after exsanguination and resuscitation.12 This activity can be blocked by the destruction of both the amygdala but not of the cerebral cortex, suggesting that the amygdala may serve as pacemakers after diffuse anoxic-ischemic insult, driving in turn the thalamus, caudate and the cortex. After a midbrain or thalamic lesion, there is a de-afferentation of thalamo-cortical circuits, releasing the autonomous cortical alpha frequency generators from the ascending arousal influences of the reticular activating system.13 The evolution of EEG patterns in coma has not been systematically studied. In 1 patient with cardiorespiratory arrest, Scott and Sumra found an initial alpha pattern with supervening beta activity which evolved to a spindle pattern and finally to an iso-electric tracing over a 7-day period.14 In another patient with fatal post-cardiorespiratory arrest coma, 6 serial EEGs showed transition from alpha pattern to theta activity over 11 days.15 In both these cases, it is evident that a transition from faster to slower frequencies occurred over several days and the patients ultimately died. In our case, the transition occurred from a predominantly beta activity to an alpha pattern and subsequently, the patient died. It appears that such transition to slower frequencies might reflect progressive neurological deterioration and might serve as an adverse prognostic factor. To conclude, it is likely that, following anoxic brain injury, the frequency of the abnormal EEG rhythm may include not only the well-recognized alpha and theta range, but also a predominantly beta range, especially in children. The evolution of the EEG pattern from faster frequency activity (delete?) to one of slower frequency may be a poor prognostic indicator reflecting progressive neurological deterioration. REFERENCES 1. Chatrian G. Coma and other states of altered responsiveness and brain death. In: Daly DD, Pedley TA, editors. Current Practice of Clinical Electroencephalography. New York: Raven Press; 1990, pp. 442-3.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03083f1.jpg] [ni03083f2.jpg] |
| |||||||||

{kind=link}
{kind=link}