 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
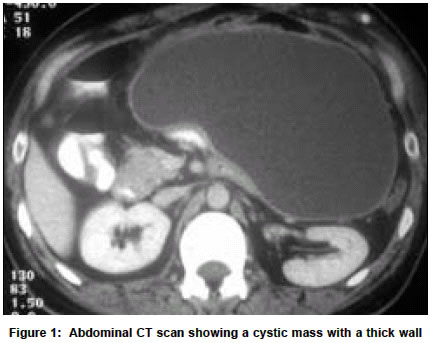
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 269-270 Case Report Laparoscopic management of complicated ventriculoperitoneal shunts S. Jain, D. Bhandarkar, R. Shah,* U. Vengsarkar Sir Hurkisondas Nurrottumdas Hospital & Research Centre, Padmashri Gordhanbapa Chowk, Raja Rammohan Roy Road, Mumbai-400004 and *Jaslok Hospital & Research Centre. Deepraj Bhandarkar Accepted on 07.09.2001. Code Number: ni03084 ABSTRACT Intra-abdominal migration of the catheter and formation of a cerebrospinal fluid pseudocyst are both rare complications of a ventriculoperitoneal shunt. Traditionally, each condition is treated by a formal laparotomy. Laparoscopic management of the complications in two patients is described. Key Words: Hydrocephalus, Laparoscopy, Ventriculoperitoneal shunt, Shunt malfunction cerebrospinal fluid pseudocyst. In the decade since the introduction of laparoscopic cholecystectomy, the applications of laparoscopic surgery have expanded tremendously. Today, surgeons facile with laparoscopic surgery can use the technique to treat a variety of conditions outside the purview of general abdominal surgery. In this paper we describe two patients, one with abdominal migration of a ventriculoperitoneal (VP) shunt and the other with an abdominal cerebrospinal fluid (CSF) pseudocyst, treated by laparoscopic surgery. To the best of our knowledge, this is the first report describing the use of laparoscopy in the management of complicated VP shunts, from an Indian center. CASE REPORT Case 1 A 40-year-old man presented with features of raised intracranial tension (ICT). He had undergone placement of a VP shunt several years ago. An abdominal X-ray showed intraperitoneal migration of the entire catheter, later confirmed by CT scan. Both the neurosurgical and laparoscopic teams participated in the operation performed under general anesthesia. Open laparoscopy was used to place a 10 mm laparoscopic cannula in the peritoneal cavity through an infraumbilical incision, and the abdomen was insufflated with CO2 to a pressure of 12 mm Hg. Laparoscopic examination revealed the catheter to be lying free atop loops of the small bowel. A second 5 mm cannula was inserted in the right iliac fossa, the catheter was picked up with a grasping forceps and the entire assembly including the cannula was withdrawn from the abdomen. The retrieved catheter was inspected to exclude any damage and flushed with saline to confirm its patency. At this point, the abdomen was desufflated leaving the 10 mm cannula in place. The neurosurgical team re-explored the scalp incision to expose and free the Y-connector of the cephalic pump. An introducer inserted subcutaneously from the inferior angle of the scalp incision was made to emerge from the 5 mm incision in the right iliac fossa. The catheter was attached to the introducer, withdrawn into the occipital wound and secured to the Y-connector. The abdominal end of the catheter was then reintroduced into the peritoneal cavity via the track of the 5 mm cannula. The abdomen was reinsufflated and the laparoscope reintroduced to confirm satisfactory positioning of the catheter tip in the pelvis and free flow of the CSF. Postoperatively, and at the follow-up of 8 months, the patient was well. Case 2 A 38-year-old man who had bilateral VP shunts in place presented with a progressively expanding upper abdominal mass, fever and signs of raised ICT. He had previously undergone three shunt revisions over a 13-year period. On admission, the patient was febrile, had tachycardia and was drowsy. Abdominal examination revealed a large, non-tender, immobile mass with a smooth surface and soft consistency extending from the left upper quadrant to the umbilical region. Hematological and biochemical parameters were normal except a total leucocyte count of 18,000 / cu mm with 82% polymorphs. An abdominal CT scan revealed a cystic mass with a thick wall (Figure 1). The cyst was aspirated under CT guidance and a liter of straw-colored fluid was aspirated. Smear examination with gram staining and culture of the fluid were negative. After commencing intravenous antibiotics, the patient's pyrexia subsided and neurological status improved. However, abdominal sonography performed a week later showed the cyst to have refilled to its original size. At this juncture, a decision was made to drain the CSF pseudocyst laparoscopically and salvage the malfunctioning VP shunt catheter. The laparoscopic operation was performed under general anesthesia using one 10 mm and two 5 mm cannulas. After preliminary inspection, omentum covering the cyst was dissected and a large portion of the cyst wall was excised to drain the contents into the peritoneal cavity; the excised portion was submitted for histopathological examination. The internal, flimsy fibrinous septae were broken and the cyst cavity was irrigated. An incision was made over the parietal peritoneum in the left iliac fossa to identify and retrieve the VP shunt catheter. The tip of the catheter was placed in the pelvis after confirming its patency. The previously placed right-sided VP shunt catheter was also identified and omentum wrapped around its tip was teased away. This catheter was directed towards the right subdiaphragmatic region. He was admitted to the intensive care unit and was treated with antibiotic therapy and mechanical ventilation, and both the VP shunts were exteriorized. However, he suffered bilateral aspiration pneumonitis and succumbed to sepsis some 14 days later. DISCUSSION Disconnection of the shunt and migration of the tube into the peritoneal cavity is an uncommon complication. In 1976, Davidson reviewed 356 patients and identified 11 with peritoneal migration of shunt parts.1 Until now retrieval of a migrated catheter has necessitated a formal laparotomy. Laparoscopic retrieval of catheter parts accomplished through incisions totalling about 1.5 cm_2 cm in length and with the help of delicate instruments can be expected to minimize the risk of a laparotomy and the formation of intraperitoneal adhesions. Furthermore, laparoscopy allows visual confirmation of the adequate flow of the CSF from the end of the catheter after it is repositioned. However, the greatest advantage of laparoscopy lies in its ability to assess the entire abdominal cavity for the presence of adhesions and undertake adhesiolysis whenever necessary. This allows placement of the catheter in the quadrant of the abdomen with the maximum absorptive surface. Harsh, in 1954, first described a CSF pseudocyst, an intra-abdominal collection of CSF, as a rare complication of VP shunting.1 The incidence of this condition varies from 1% to 4.5%.2 In 1994, Rainov et al reviewed 115 cases from the literature, and added 14 of their own.3 A CSF pseudocyst is thought to arise as a result of the reaction of the intraperitoneal structures to either the catheter itself or to the CSF. The factors incriminated in the etiology include shunt infection, subclinical peritonitis, previous laparotomies, high protein content of the CSF and a malabsorption syndrome associated with an antigen-antibody reaction after immunization.4 We could identify only two previous reports of laparoscopic drainage of a CSF pseudocyst in the surgica literature. Kim et al excised a portion of a CSF pseudocyst, removed the shunt catheter from the residual cavity and repositioned it within the peritoneal cavity in a 12-year-old boy.5 There was no recurrence after 12 months of follow-up. Brunori et al performed a laparoscopic drainage of a pseudocyst containing 2 liters of fluid and retrieved the catheter from the peritoneal cavity.6 In our patient laparoscopy proved useful not only for draining the pseudocyst but also for salvaging the catheters. REFERENCES 1. Harsh GR. Peritoneal shunt for hydrocephalus utilizing the fimbria of the fallopian tube for entrance to the peritoneal fluid. J Neurosurg 1954;11:284-94. Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03084f1.jpg] |
| |||||||||

{kind=link}