 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
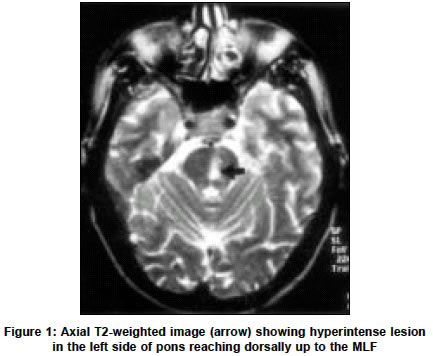
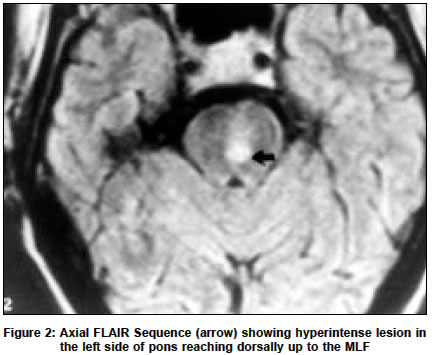
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 271-272 Case Report Internuclear ophthalmoplegia and torsional nystagmus: An MRI correlate A. K. Srivastava, M. Tripathi, S. B. Gaikwad,* M. V. Padma, S. Jain Departments of Neurology and *Neuroradiology, Neurosciences Center, All India Institute of Medical Sciences, New Delhi-110029. Achal K. Srivastava Accepted on 05.06.2001. Code Number: ni03085 ABSTRACT The association of internuclear ophthalmoplegia (INO) with torsional nystagmus is rare. We report a case of a 72-year-old male who developed brainstem stroke and was found to have left INO with torsional nystagmus. An MRI correlation in this case has been described. Key Words: Torsional nystagmus, Brainstem, Ophthalmoplegia. Internuclear ophthalmoplegia (INO) is of considerable value in anatomic and etiologic diagnosis. INO occurs in a primary brainstem lesion. INO may be bilateral or unilateral. The bilateral form is more common and is usually due to multiple sclerosis. Unilateral INO is uncommon and is usually related to an infarct of the brainstem in the older age group.1 The association of INO with torsional nystagmus is rare and only a few cases have been reported in the literature.2-4 CASE REPORT A 72-year-old man was admitted with complaints of sudden onset dizziness and vomiting. Examination revealed a high blood pressure (200/120 mm Hg). There was no history of visual loss, diplopia, dysarthria, dysphagia, and loss of consciousness or headache. The patient was non-diabetic and did not have any other risk factor for stroke. Neurological examination revealed left INO: adduction paralysis at left eye and normal convergence with abduction nystagmus in right eye. In the mid-position there was clockwise torsional nystagmus. On right gaze the nystagmus increased in amplitude superimposed on abduction nystagmus. There was no skew deviation and head tilt. There was incoordination in left upper limb and mildly impaired knee heel test in left lower limb. The rest of the neurological examination was unremarkable. Non-contrast computerized tomography (NCCT) of brain done at 6 hours after the onset of symptoms was normal. The patient was placed on low molecular weight heparin (0.4 ml, 12 hourly). Magnetic resonance imaging was done on the fifth day. T2weighted axial image (Figure 1), T2-weighted sagittal image, and FLAIR sequence (Figure 2) revealed hyperintense signal in the left upper pons which was extending right up to the medial longitudinal fasciculus (MLF). T1-weighted axial images showed hypointensity in the corresponding region of pons. DISCUSSION Pontine lesions may lead to lateral eye movement disturbances: INO, paramedian pontine reticular formation (PPRF) syndrome or abducens nucleus syndrome. Combinations of these symptoms are sometimes referred to as one-and-a-half syndromes.5 PPRF at the level of abducens nucleus constitutes the center for horizontal gaze. The pontine center commands lateral gaze by the simultaneous innervation of the ipsilateral lateral rectus muscle and the contralateral medial rectus through the MLF. Unilateral lesion of the MLF between the midpons and the oculomotor nucleus disconnects the ipsilateral medial rectus subnucleus, producing adduction failure during horizontal gaze. The latter, in association with abduction nystagmus of the opposite eye is called INO. INO is a definite sign of intrapontine or mesencephalic lesion. The nystagmus has been postulated to reflect impaired inhibition in the medial rectus muscle of the abducting eye. The association of INO with torsional nystagmus is rare.2-4 Lopez et al, in a review of 35 cases of torsional nystagmus, found lesions in the vestibular nuclei.6 INO was not seen in any of the cases. Noseworthy et al reported a case of counterclockwise torsional nystagmus in a patient with left midpontine lesion.7 It was also associated with minor slowing of adduction at the left eye and hypertropia at the left eye. Torsional nystagmus generally accompanies horizontal nystagmus due to labyrinthine disease. Pure torsional nystagmus is a rare form of central vestibular nystagmus and is attributed to an imbalance of central vestibular projections from the vestibular nuclei to the midbrain nuclei. Pure torsional nystagmus may be seen with brainstem lesions such as syringobulbia, syringomyelia with Arnold-Chiari malformation, lateral medullary syndrome, multiple sclerosis and vascular anomalies. Large amplitude torsional nystagmus may accompany thalamic lesions and underlies the abnormality described with seesaw nystagmus.8 In the torsional nystagmus quick phase is always ipsilesional. The interstitial nucleus of cajal (INC) is the integrator for ipsiversive torsional movements. The INC is situated between the red nucleus and the superior colliculus. It is proposed that INC inactivation produces a contralesional torsional deviation and a torsional ipsilesional nystagmus.9 The INC receives excitatory inputs from the vertical semicircular canals of the contralateral labyrinth via the MLF. Projections from the vestibular nuclei or vestibulocerebellum to the INC coordinate torsional gaze. An MLF lesion could produce inactivation of the INC. The ipsilateral rostral interstitial nucleus of MLF (riMLF) generates ipsilesional saccades and if involved produces contralesional ocular tilt reaction. In the present case MRI of the patient revealed a small infarct in the left upper pons that was extending up to the MLF. There were no lesions in the vestibular nuclei and INC. The mesencephalon was intact. The above lesion involving the MLF could be responsible for the inactivation of the ipsilateral INC inducing a contraversive slow phase. The presence of a corrective ipsiversive quick phase points towards an intact riMLF. REFERENCES 1. Gonyea EF. Bilateral internuclear ophthalmoplegia. Arch Neurol 1974;31:163-73.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03085f1.jpg] [ni03085f2.jpg] |
| |||||||||

{kind=link}
{kind=link}