 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
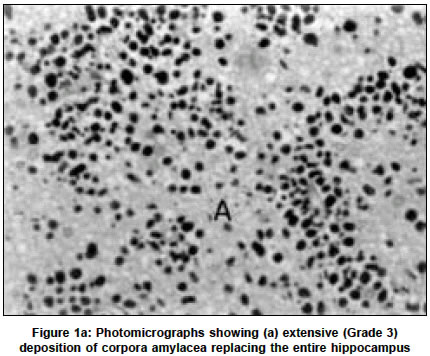
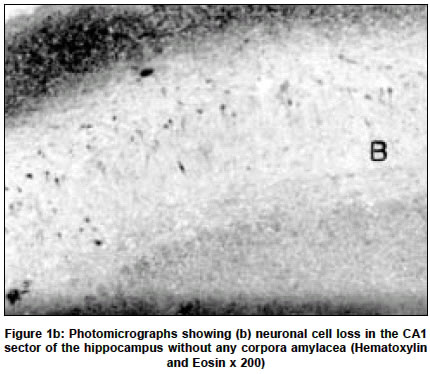
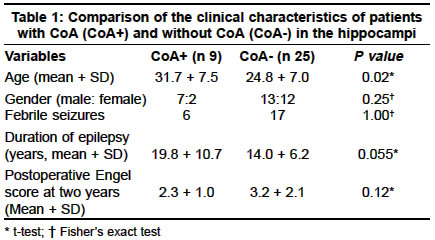
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 277-278 Short Report The significance of corpora amylacea in mesial temporal lobe epilepsy P. Joseph Cherian, V. V. Radhakrishnan, K. Radhakrishnan R. Madhavan Nayar Center for Comprehensive Epilepsy Care and Department of Pathology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum-695011, India. K. Radhakrishnan Accepted on 31.01.2002. Code Number: ni03089 ABSTRACT Temporal lobe epilepsy (TLE) associated with mesial temporal sclerosis (MTS), mesial TLE (MTLE), is the commonest medically refractory adult epilepsy syndrome. Corpora amylacea (CoA) have been shown to be a marker of MTS. We compared 9 patients with MTS who had dense deposition of CoA in their hippocampi with 25 patients with MTS who did not have CoA. The patients with CoA were significantly older and they showed a trend towards having a significantly longer duration of epilepsy. The postoperative seizure outcome at 2 years was not different in the 2 groups. Our results could indicate the progressive nature of the pathology of MTS, probably indicating excitotoxic damage due to recurrent seizures, but they need to be verified by clinicopathological correlation among a larger number of patients with MTLE. Key Words: Corpora amylacea, Epilepsy surgery, Mesial temporal sclerosis, Temporal lobe epilepsy. The most common pathologic lesion, seen in over two-thirds of the adult patients with medically refractory temporal lobe epilepsy (TLE) is mesial temporal sclerosis (MTS).1 MTS is characterized by selective neuronal loss and reactive gliosis in the hippocampus, predominantly involving the CA1, CA3 and CA4 sectors of the cornu ammonis (CA) of the hippocampus and other mesial temporal lobe structures.2 TLE with histopathologically confirmed MTS, mesial TLE (MTLE), is a strong predictor of a favorable seizure outcome following anterior temporal lobectomy (ATL).3 In surgical specimens that are not resected en bloc, estimating the neuronal loss as well as describing the pathologic changes in various subdivisions of the hippocampus is often difficult. In this context, identification of other markers of MTS becomes important. Although CoA are often seen in a variety of neurodegenerative disorders and in the brain of elderly normal individuals, their abundant accumulation in the pyramidal layer of the CA1 sub-region of the hippocampus has recently been documented to be a distinctive marker of MTS.1,4,5 We undertook the present study to inquire if there were differences in the clinical characteristics between MTLE patients who did and who did not have CoA in their hippocampi. Our hypothesis was that a dense deposition of CoA in the hippocampus would suggest a more advanced MTS and therefore might be correlated with a longer duration of TLE and with a more favorable postoperative seizure outcome. MATERIAL AND METHODS We have already reported in detail the neuropathological features of the first 100 consecutive patients who underwent ATL at the Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, for medically refractory TLE.1 Among the 58 patients of this group with pathologically verified MTS, 33 had and 25 did not have CoA in their hippocampi. We defined MTS in the surgical specimens as hippocampal neuronal loss or gliosis or both seen on hematoxylin and eosin staining.1 The sections of hippocampus and temporal neocortex were also stained with Luxol fast blue - Periodic acid Schiff's stain to highlight the distribution of CoA. The presence of CoA in the CA1 and CA3 regions, dentate gyrus, and end folium of the hippocampus in all the specimens was scored on a semi-quantitative scale and was graded as: >10 CoA per high power field (HPF) (Grade 3), 6-10/HPF (Grade 2), <5/HPF (Grade 1) and none (Grade 0). Nine patients out of 33 patients with Grade 3 CoA deposition (Figure 1a) in the hippocampi formed the CoA+ group and 25 patients without CoA (Figure 1b) formed the CoA- group for this study. The demographic and seizure characteristics of the CoA+ and CoA- groups, and their seizure outcome, as measured by the Engel Score3 at 2 years following ATL, were compared using the Student's t-test or Fisher's exact test, as appropriate. We used mean + standard deviation to define the dispersion. A P value of <0.05 was considered as significant. RESULTS Table 1 depicts the variables compared between the CoA+ and CoA- groups and their significance. The mean age at ATL of the patients in the CoA+ group differed significantly from that of the CoA- group (31.7 + 7.5 years versus 24.8 + 7.0 years, P 0.02). The mean duration of epilepsy prior to ATL in the CoA+ patients was 19.8 + 10.7 years and in the CoA- patients was 14.0 + 6.2 years (P 0.055). The postoperative mean Engel score at 2 years of 2.3 + 1.0 of the CoA+ group did not differ from the score of 3.2 + 2.1 of the CoA- group (P 0.115). Other variables such as gender and past history of febrile seizures also did not differ between the two groups. DISCUSSION The significant finding of this study was that among patients with medically intractable MTLE undergoing ATL, those patients with MTS and dense deposition of CoA in their hippocampi tend to be older. Although CoA are well known to occur during the course of normal aging, the mean age of the CoA+ group was 32 years. Furthermore, their sparse deposition in the subpial regions seen in aged brains is very much different from the dense deposition seen in the CA1 and CA3 regions of the hippocampi of patients with MTLE.1,4,5 The peculiar pattern of the distribution of CoA correlating with the distribution of the neuronal loss in the hippocampus in MTS with maximal affection of the CA1 and CA3 regions and relative sparing of the CA2 region, suggests a common pathogenetic mechanism.1,2 The selective vulnerability of the CA1 and CA3 regions has been attributed to an excitotoxic mechanism probably related to the high density of glutamate binding sites and relatively small concentrations of calcium buffering proteins like calbindin and chromogranin A in these regions.2 A recent neuroimaging study6 has shown that recurrent seizures could result in continued neuronal loss and progression of the lesion in MTS. Based on these facts, it may be hypothesized that patients with MTS and more dense deposition of CoA would have a longer duration of epilepsy as compared to patients with MTS and no CoA. Our results showed a trend in that direction, but did not attain statistical significance (Table 1). We found no significant difference in seizure outcome at 2 years following ATL between patients with and without CoA. We deliberately chose patients with MTS who had a dense deposition of CoA in their hippocami for this pilot study in order to define a homogenous and well-characterized group, but thereby could have biased the sample. The small number of patients in both groups also could have compromised the results. Because of these limitations, our preliminary observations required to be verified utilizing a larger number of patients. REFERENCES 1. RadhakrishnanVV, Rao MB, Radhakrishnan K, et al. Pathology of temporal lobe epilepsy: an analysis of 100 consecutive surgical specimens from patients with medically refractory epilepsy. Neurol India 1999;47:196-201.
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03089f1a.jpg] [ni03089f1b.jpg] [ni03089t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}