 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
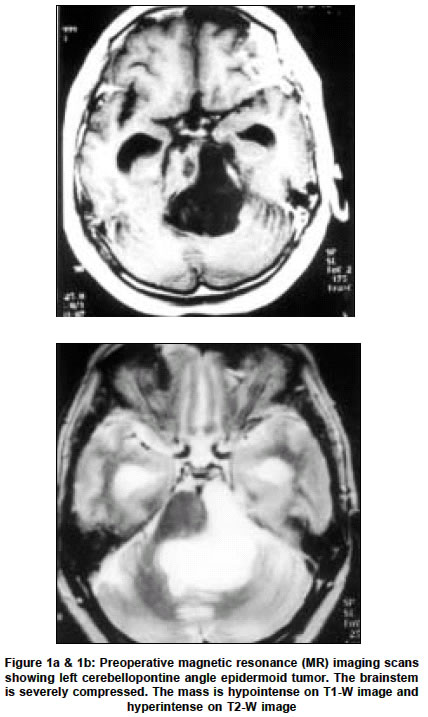
Neurology India, Vol. 51, No. 2, April-June, 2003, pp. 288 Letter to Editor Cerebellopontine angle epidermoid tumor presenting with hemifacial spasms K. Desai, T. Nadkarni, R. Bhayani, A. Goel Accepted on 24.06.2002. Code Number: ni03097 Sir, Hemifacial spasms are rarely associated with cerebellopontine angle mass lesions.1 In the majority of cases with hemifacial spasm, the well-known cause remains the vascular compression at the root entry zone of the facial nerve.2 Although rare, hemifacial spasm is associated with etiological factors other than compression by a vessel. Epidermoid tumors are among the common cerebellopontine angle tumors reported in association with hemifacial spasm.3 Ninety-five cases of cerebellopontine angle epidermoid tumors were operated in our department from 1976 to 2000. Four patients amongst these presented with hemifacial spasm. There were 3 females and 1 male patient. The age ranged from 28 to 42 years (mean 34.5 years). The duration of symptoms varied from 2 years to 6 years (mean 3.5 years). The clinical features are summarized in Table 1. One of these patients, had tinnitus and trigeminal neuralgia in addition to hemifacial spasm. Preoperatively all 4 patients had a Magnetic Resonance (MR) imaging scan. The lesions were isointense on T1-weighted sequences and were uniformly hyperintense on T2-weighted sequences in relation to the brain tissue (Figures 1a & 1b). Accurate preoperative diagnosis of the epidermoid tumor was possible in all 4 patients on MR scan. All the epidermoid tumors were located in the cerebellopontine angle on the side of the hemifacial spasm. The tumors were approached by a retromastoid craniectomy. In all 4 patients a radical excision was performed leaving behind only those remnants of the tumor capsule densely adherent to the neurovascular structures and the brainstem in the cerebellopontine angle. In 3 cases, the anterior inferior cerebellar artery (AICA) loop was noted to indent the 7th-8th cranial nerves complex and a microvascular decompression was performed after the tumor excision. In the fourth case the vascular loop had no close relationship to the 7th-8th cranial nerves complex. After surgery all 4 patients were relieved of their hemifacial spasms and other irritative neural symptoms. Postoperative MR scans confirmed radical excision of the epidermoid tumor. The follow-up ranged from 1 year to 3 years (mean 2.2 years) and all patients were free of symptoms except persistent hearing loss in 1 patient. Hemifacial spasm is assumed to be due to compression by a vascular loop at the root entry zone of the facial nerve. Common among them are the posterior inferior cerebellar artery, anterior inferior cerebellar artery and vertebral artery.4 The crucial site for compression is the junction of the glial and non-glial portion of the affected nerve.4 The excellent result following microvascular decompression confirms the vascular etiology of hemifacial spasm in the majority of cases.4 However, rarely hemifacial spasms can occur due to intracranial mass lesions, aneurysms or ectasia of the basilar arteries or its branches.1 The common intracranial tumors producing hemifacial spasms are epidermoid, meningioma, acoustic neurinoma and rarely facial neurinoma, trigeminal neurinoma and lipoma.1,5 Epidermoid tumor is one of the common tumors in the cerebellopontine angle to produce hemifacial spasm. The incidence of the occurrence of hemifacial spasm in the cerebellopontine angle epidermoid tumor ranges from 0.3% to 1.2 %.3 There are isolated case reports of epidermoid tumors in the cerebellopontine angle.1,3 Various pathomechanisms have been proposed for the development of hemifacial spasm. The compressive effect on the nerve by the intracranial tumor or a vascular loop leads to focal demyelination and the resultant formation of false synapses. Aberrant transmission of nerve impulses occurs through these false synapses and a peripheral reverberating circuit is set up between afferent and efferent fibers at the site of the compression. Ectopic excitation results in ephaptic transmission and hemifacial spasm. The focal compression also results in increased interstitial resistance in the para axonal space. The surgical decompression of the nerve reduces this resistance and abolishes aberrant excitation. Microvascular decompression is known to have excellent clinical results and can also cause remyelination of the nerve fibers. Epidermoid tumor may also cause irritation of the facial nerve by its irritant contents like keratin and cholesterol.6 There is a debate as to whether microvascular decompression of the facial nerve is required following excision of the epidermoid tumor. In our series 3 patients had a vascular loop indenting the facial nerve. Microvascular decompression was done in these patients and the results were excellent. In cases where the vascular loop is not closely related to the facial nerve, microvascular decompression is not necessary and the results are equally satisfactory.3 REFERENCES 1. Nagata S, Matsushima T, Fujii K, et al. Hemifacial spasm due to tumour, aneurysm or arteriovenous malformation. Surg Neurol 1992;38:204-9. Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03097t1.jpg] [ni03097f1.jpg] |
| |||||||||

{kind=link}
{kind=link}