
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 51, Num. 3, 2003, pp. 350-354
|
Untitled Document
Neurology India, Vol. 51, No. 3, July, 2003, pp. 350-354
Effect of mannitol in experimental spinal cord injury: An ultrastructural and electrophysiological study
Baysefer A, Erdogan E, Kahraman S, Izci Y, Korkmaz C, Solmaz I, Ulas UH, Ozogul C, Timurkaynak E
Departments of Neurosurgery, Gülhane Military Medical Academy, 06018 Etlik-Ankara
Correspondence Address:
Department of Neurosurgery, Gülhane Military Medical Academy, 06018 Etlik-Ankara
eerdogan@gata.edu.tr
Code Number: ni03114
ABSTRACT
Background: Although many experimental and clinical studies were performed on the pathophysiology and treatment of spinal cord injury (SCI), the electrophysiological and ultrastructural changes of the spinal cord were not precisely evaluated. Aims: To investigate the effect of mannitol on Somatosensory Evoked Potentials (SSEP), postoperative neurological recovery and ultrastructural findings after an experimental SCI. Setting: The experimental microsurgery laboratory of a university hospital. Design: A prospective, randomized animal study. Material and Methods: Sprague-Dawley rats were used and divided into three groups (Groups I-III) for this study. Those in Group I were control animals who underwent laminectomy only, and non-traumatized spinal cord samples were obtained 2 weeks later. SCI was produced in Groups II and III using clip compression technique, and cord samples were obtained 2 weeks later. The rats in Group II received 2 g/kg of 20% mannitol intraperitoneally, immediately and three hours after trauma was induced; and those in Group III received the same amount of 0,9% NaCl in the same manner. Preoperative and postoperative SSEP records at the end of 2 weeks were obtained. Electron microscopy examination of the cord samples was done at 2 weeks postoperatively. Statistical Analysis used: Fischer's Exact Test. Results: SSEP records, ultrastructural findings and clinical recovery showed that minor neural damage and significant recovery occurred in Group II. Conclusion: This study demonstrates that the administration of 2 g/kg of 20% mannitol produces significant improvement in the neural structures and protects the spinal cord following injury.
INTRODUCTION
After a traumatic injury to the spinal cord, there is evidence that spinal cord injury (SCI) in the acute phase is caused by two separate mechanisms: the initial mechanical damage and secondary changes due to vascular or biochemical effects.[1] Within a few minutes of the injury signs of cellular damage appear. Subsequent to cellular changes there is destruction of the spinal cord tissue, an inflammatory response and edema, and also a decrease in the spinal cord blood flow.[2] Functional losses of the spinal cord are more often due to secondary changes than due to morphologic primary damage.[3]
Mannitol, a hyperosmolar agent, has been used in neurosurgical practice for many years to reduce intracranial pressure (ICP).[4] Mannitol has demonstrated a positive effect on cerebral microcirculation and improvements in cerebral blood flow (CBF) have been shown to occur with the administration of mannitol after vessel occlusion.[5] Furthermore, mannitol has been implicated as a potent inhibitor of free radical-mediated ischemic cell damage; its role as a scavenger of oxygen-derived free radicals and, in particular, of the hydroxyl radical has been repeatedly emphasized in a number of experimental studies.[6],[7]
Our aim is to investigate the effect of mannitol on rats with a damaged spinal cord, clinically, electrophysiologically and ultrastructurally.
MATERIAL AND METHODS
Animal preparation
After receiving approval from the Gulhane Military Medical Academy ethics committee, the experiments were conducted using male Sprague-Dawley rats weighing 250 to 300 g. The animals were randomly assigned to three groups. The surgical procedure was performed after general anesthesia was induced by a combination of 10 mg/kg xylazine (Rompun,Bayer, Germany) and 30 mg/kg ketamine hydrochloride (Parke Davis, England) administered intramuscularly. Ketamine was used for anesthesia because it has a poorer recovery level relative to the other anesthetic protocols in the management of SCI.8 Following the anesthesia, each rat was pinned in the prone position and its back was shaved. After a midline thoracic incision and blunt separation of paravertebral muscles from the spinal column, laminectomy was performed between T6 and T7 under a surgical microscope (Opmi 3, Zeiss, Germany) and temporary aneurysm clips with a closing force of 50 gr (Codman-Sundt Slim Line) were applied extradurally for 10 seconds between the T6 and T7 levels of the spinal cords of rats in Groups II and III.
Description of groups
First all animals' preoperative Somatosensory Evoked Potentials (SSEP) (Key Point SSEP recording unit) records were achieved as normal SSEP values and postoperative records were also obtained at the end of 2 weeks before sacrificing the animals. In the rats of Group I (10 sham-operated controls) only laminectomy was performed, and 0.5 cm of non-traumatized spinal cord was obtained 2 weeks postoperatively. The rats in Group II (20 mannitol treatment group) received 2 g/kg of 20% mannitol intraperitoneally immediately and 3 hours after trauma was induced. The rats in Group III (20 trauma-induced animals) underwent surgical and traumatic interventions and received 2g/kg of 0,9% NaCl by intraperitoneal injection immediately and 3 hours after trauma was induced.
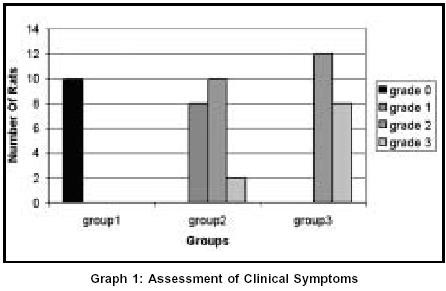
Clinical grading
The neurological situation of all animals was carefully evaluated on the day of sacrifice. Although the distinction between voluntary and involuntary movements was sometimes puzzling, the motor functions of individual rats were roughly graded as follows:9
Grade 0: No difference from normal rats
Grade 1: Crawling with mild difficulty
Grade 2: Some voluntary movement to support the hindquarters
Grade 3: No voluntary movement
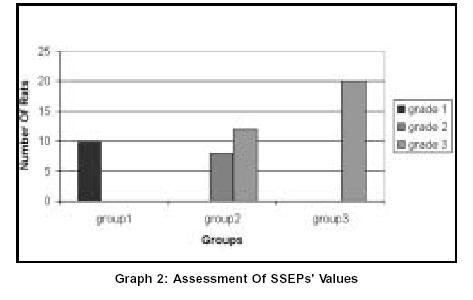
Electrophysiological grading
Preoperative and end of the experiment SSEP values of the rats were obtained. SSEPs recorded from the platinum electrode over the somatosensory cortex were elicited by applying cathodal stimuli (intensity 10 mA, pulse duration 50 msec and presentation rate 7.5 Hz) to the left sciatic nerve. All responses were recorded at a bandwidth of 20 to 2000 Hz, averaged, and replicated. Postoperatively in the third week the animals were roughly graded as follows:
Grade 1: No difference from normal rats
Grade 2: Abnormal potentials (prolonged latency and decreased amplitude)
Grade 3: No potentials
Electron microscopy examination
The tissue samples were prepared for electron microscopy as follows: the spinal cord segments were removed and placed in 2.5% glutaraldehyde for 24 hours for fixation. The tissue was postfixed with OsO4, dehydrated in a graded series of alcohol, and then embedded in Araldit CY212. Semi-thin sections (2 micrometer) were stained with toluidine blue and observed on light microscopy. The thin (60-90 nm) sections were obtained with ultra-microtome (Reichert Supernova) and stained with uranyl acetate and lead citrate, examined on a transmission electron microscope (TEM) (Zeiss EM 900), and photographed.
Statistical Analysis
The statistical significance of the clinical and electrophysiological grading between the groups was defined using Fischer's Exact
Test.
RESULTS
Neurological examinations
Clinical grading of individual animals is shown in Graph 1.
The average score of the animals on day 14 was 1.7 for Group II and 2.4 for group III. There were statistically significant differences in the clinical grading between the mannitol-treated group and the trauma- alone group (P<0.003).
Electrophysiological evaluation
The SSEP grading of individual animals is shown in Graph 2. The SSEP values of all animals of Group I were the same as preoperative values (Grade I). There was no change of latency and amplitude data in this group. The average score of the animals on Day 14 was 2.4 for Group II and 3 for Group III. There were statistically significant differences in the electrophysiological grading between the mannitol-treated and the trauma-only animals (P<0.003).
Ultrastructural findings
Group I (Sham-operated group)
Normal ultrastructural findings were seen in the spinal cord samples obtained in all the control rats [Figure-1]. Homogeny in the axonal cytoplasm and myelin sheaths' covering axons could be seen. Myelin sheaths' thickening and axonal size were normal. Normal mitochondrion and cristae structure could be seen in the axonal cytoplasm.
Group II (Mannitol-treated group)
The existence of axonal degenerations and tractions could be seen more easily in this group's slices than in the sham-operated ones. Less axonal degenerations were found in the white matter in samples obtained from the mannitol-treated rats than the trauma-alone rats at 2 weeks post-injury. The displacement of the axonal cytoplasm was seen in nearly each fiber. The swollen mitochondria were abundant, and a few mitochondria had cristae. The thin myelin sheath was mainly observed in samples obtained at 2 weeks post-injury [Figure-2]. The myelin was characterized by clefts between the myelin layers.
Group III (Trauma-alone group)
Abnormal axons were observed in the white matter of the specimens obtained from the trauma-alone rats at two weeks post-injury. The most typical axonal change observed in the white matter was prominent edema in the axoplasma. The neurofilaments and vesicles were sparse, and there were large areas of clearing. Some of the fibers with an empty appearance were associated with axonal displacement. The edematous mitochondria usually did not include cristae. The surrounding myelin sheath was slender and cracked. The myelin clefts between the myelin layers were abundant. The vesiculated myelin frequently extended into the extracellular space. Some fibers lost their myelin cover and also cytoplasmic organelles [Figure-3]. All these changes were rare or absent in the control group.
DISCUSSION
A number of laboratories employing anatomical, biochemical and physiological methods have documented a decrease in spinal cord microvascular patency and ischemia beginning within minutes following severe contusion or compression injury. These investigatons have reported that the free radical-induced lipid peroxidation is the most important factor precipitating posttraumatic degeneration in the spinal cord.[10],[11] Much damage to the spinal cord is due to secondary phenomena. Secondary injury has been defined as an injury to a neuron and its supporting cells which is delayed and follows a primary neurological insult by a finite period of time. This injury results in a cell dropout (death), which is greater than that observed with the primary injury alone.[12] The treatment protocols of SCI are based on stopping or reversing such a mechanism at any step; there is no surgical or medical treatment for primary damage, but it is possible to block the secondary damage. Therefore, the inhibition of lipid peroxidation by many agents, such as antioxidants or free radical scavengers given in large doses, may be useful.[13] GM 1 gangliosids, selenium, melatonin, naloxane, alpha-tocopherol, seratonin 1A agonists and mexiletine are the other agents that were widely examined in experimental SCI models.[14],[15]
The mechanism of mannitol has primarily been related to the osmotic dehydration of the brain secondary to a reduction in cerebral water content. Additionally, mannitol has been shown to increase the cerebral blood flow (CBF) due to a transient hypervolemia, decrease the blood viscosity due to hemodilution and alter red blood cell deformability. These effects ultimately improve oxygen delivery at the cerebral arterioles, which allows a decrease in cerebral blood volume (CBV), and therefore a decrease in the ICP.[16] Furthermore, mannitol has been implicated as a potent inhibitor of free radical-mediated ischemic cell damage; its role as a scavenger of oxygen-derived free radicals and, in particular, of the hydroxy radical has been repeatedly emphasized in a number of experimental studies.[6],[7]
Although mannitol has been used in head traumas for many years, Magnaes reported the case of a patient with SCI who was treated with mannitol in 1977.[17] Parker et al showed that reduced spinal cord edema was seen with mannitol therapy after experimental SCI in dogs in 1973.[18] Electrophysiology, including evoked potentials, has been widely used as a non-invasive parameter of spinal cord function. Reed et al conducted an experimental study on the effect of mannitol (3 g/kg) on SCI and stated that mannitol therapy did not reverse the loss of the cortical evoked response observed during the 4-hour interval studied, but the observation of improved blood flow patterns in the white matter is encouraging and warrants further study.[19] In 1989 Dyste et al compared the effects of mannitol, hetastarch and phenylephrine on the spinal cord blood-flow following experimental SCI.[20] They used 1g/kg of mannitol as a therapeutic dose, recorded the SSEP, cardiac output, mean arterial pressure, hematocrit of each group and performed a histological examination of the injured site. They concluded that mannitol caused a transient but significant increase in the cardiac output and a significant fall in hematocrit. But it did not improve the spinal cord blood flow and did not cause any histological change at the injured site. The effect of mannitol in the treatment of SCI has also been investigated by Isu in 1990.[21] He used 2 g/kg of mannitol with intravenous bolus injection and showed a transient recovery in the spinal cord evoked potentials of the group treated with mannitol. In his other study, he compared the effects of mannitol and myelotomy and suggested that mannitol has a significant but transient effect on the recovery.[22] Although there is no consensus on the therapeutic dose of mannitol in the management of SCI, we administered 2 g/kg of 20% mannitol because it is the lowest effective dose of mannitol reported in the literature.
Although many methods of histological examination have been used to evaluate the effects of neuroprotective agents on the spinal cord, electron microscopy examination is not widely used for the evaluation of the effectiveness of pharmacotherapy. Recently, Kaptanoglu et al proposed a grading system according to ultrastructural findings including axonal myelin, axonal edema, axoplasmic edema, intranuclear changes and vascular endothelial edema.[23] In our study, we investigated the effect of mannitol on the SSEP and ultrastructural pattern of SCI induced with clip-compression technique in rats. We compared the ultrastructural findings of the mannitol-treated group and the non-treated group and observed fewer abnormal axons in the white matter, no clearing areas, neurofilaments in most of the axons, swollen mitochondria (a few of them had cristae), thin myelin sheath and clefts between the myelin layers in the mannitol-treated group. We also observed significant improvement in the SSEP of mannitol-treated rats. These results from the present study indicate that mannitol could provide an effective protection for the neurons. We recorded the second set of reading 2 weeks after trauma because the secondary changes in the spinal cord occur in this period. Significant ultrastructural and electrophysiological improvements were observed at the SCI site after 2 weeks. Therefore, systemic administration of mannitol may provide significant protection to the spinal cord from secondary injury after trauma.
Finally, although more experimental and clinical studies are needed to consider the use of mannitol in the treatment of patients with SCI, it does positively influence delayed neuronal injury after ischemia through its action in reducing edema in experimental animals.
REFERENCES
| 1. |
Collins WF. A review and update of experimental and clinical studies of spinal cord injury. Paraplegia 1983;21:204-19. |
| 2. |
Sandler AN, Tator CH. Effect of acute spinal cord compression injury on regional spinal cord blood flow in primates. J Nerosurg 1976;45:660-76. |
| 3. |
Anderson TE. Spinal cord contusion injury:experimental dissociation of hemorragic necrosis and subacute loss of axonal conduction. J Neurosurg 1985;62:115-9. |
| 4. |
Shenkin HA, Goluboff B, Haft H. The use of mannitol for the reduction of intracranial pressure in intracranial injury. J Neurosurg 1962;76:486-92. |
| 5. |
Andrews RJ, Bringas JR, Muto RP. Effects of mannitol on cerebral blood flow, blood pressure, blood viscosity, hematocrit, sodium, and potassium. Surg Neurol 1993;39:218-22. |
| 6. |
Shimauchi M, Yamamoto YL. Effects of retrograde perfusion of the brain with combined drug therapy after focal ischemia in rat brain. Stroke 1992;23: |
| 7. |
1805-11. |
| 8. |
Suzuki J, Imaizumi S, Kayma T, Yoshimoto T. Chemiluminescence in hypoxic brain: The second report cerebral protective effect of mannitol, vitamin E, and glucocorticoid. Stroke 1985;16:695-700. |
| 9. |
Grissom TE, Mitzel HC, Bunegin L, Albin MS. The effect of anesthetics on neurologic outcome during the recovery period of spinal cord injury in rats. Anesth Analg 1994;79:66-74. |
| 10. |
Lizuka H, Iwasaki Y, Yamamoto T, Kadoya S. Morphometric assessment of drug effects in experimental spinal cord injury. J Neurosurg 1986;65:92-8. |
| 11. |
Anderson DK, Hall ED. Pathophysiology of spinal cord trauma. Ann Emerg Med 1993;22:987-92. |
| 12. |
Anderson DK, Demediuk P. Spinal cord injury and protection. Ann Emerg Med 1985;14:816-21. |
| 13. |
Benzel EC, Wild GC. Biochemical mechanisms of posttraumatic neural injury. Perspect Neural Surg 1991;2:95-126. |
| 14. |
Anderson DK, Dugan LL, Means ED, Horrocks LA. Methylprednisolone and membrane properties of primary cultures of mouse spinal cord. Brain Res 1994;637:119-25. |
| 15. |
Kaptanoglu E, Tuncel M, Palaoglu S, Konan A, Demirpence E, Kilinç K. Comparison of the effects of melatonin and methylprednisolone in experimental spinal cord injury. J Neurosurg (Spine 1) 2000;93:77-84. |
| 16. |
Kaptanoglu E, Caner HH, Sürücü HS, Akbiyik F. Effects of mexiletine on lipid peroxidation and early ultrastructural findings in experimental spinal cord injury. J Neurosurg (Spine 2) 1999;91:200-4. |
| 17. |
Donata T, Shapira Y, Artru A. Powers K. Effect of mannitol on cerebrospinal fluid dynamics and brain tissue edema. Anest Analg 1994:78:58-66. |
| 18. |
Magnaes B. Effect of mannitol in a patient with spinal cord injury: a case report. Acta Neurochir(Wien) 1977;39:59-61. |
| 19. |
Parker AJ, Park RD, Stowater JL. Reduction of trauma-induced edema of spinal cord in dogs given mannitol. Am J Vet Res 1973;34:1355-7. |
| 20. |
Reed JE, Allen WE 3rd, Dohrmann GJ. Effect of mannitol on the traumatized spinal cord. Microangiography, blood flow patterns, and electroencephalography. Spine 1979;4:391-7. |
| 21. |
Dyste G, Hitchon PW, Girton RA, Chapman M. Effect of hetastarch, mannitol and phenylephrine on spinal cord blood flow following experimental spinal injury. Neurosurgery 1989;24:228-35. |
| 22. |
Isu T. Spinal cord evoked potential in experimental spinal cord injury; the changes in spinal cord evoked potential following impact injury. Hokkaido Igaku Zasshi 1990;65:142-51 |
| 23. |
Isu T, Iwasaki Y, Akino M, Abe H. Effect of mannitol administration and myelotomy on acute experimental spinal cord injury: investigation with spinal cord evoked potential. No Shinkei Geka 1990;18:267-72. |
| 24. |
Kaptanoglu E, Palaoglu S, Surucu S, Hayran M, Beskonakli E. Ultrastructural scoring of graded acute spinal cord injury in the rat. J Neurosurg (Spine1) 2002;97:49-56. |
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com
The following images related to this document are available:
Photo images
[ni03114g2.jpg]
[ni03114g1.jpg]
[ni03114f2.jpg]
[ni03114f1.jpg]
[ni03114f3.jpg]
|

{kind=link}
{kind=link}
![[Figure-1]](/showimage?ni/photo/ni03114f1.jpg){kind=link}
![[Figure-2]](/showimage?ni/photo/ni03114f2.jpg){kind=link}
![[Figure-3]](/showimage?ni/photo/ni03114f3.jpg){kind=link}