 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
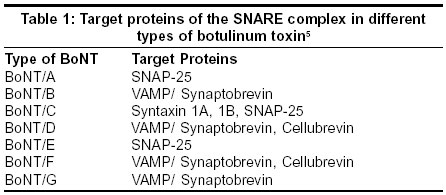
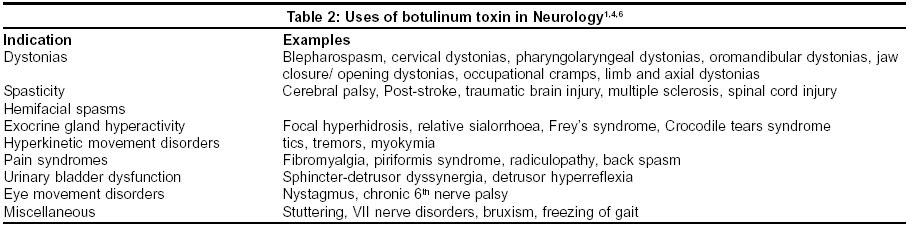
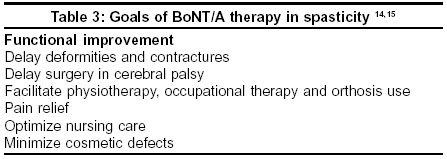
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 455-460 Review Article Botulinum toxins: Pharmacology and its current therapeutic evidence for use Muthane U, Panikar D Department of Neurology NIMHANS Hosur Road, Bangalore - 560029 Code Number: ni03150 Abstract Botulinum toxins are, as a group, among the most potent neuromuscular toxins known, yet they are clinically useful in the management of conditions associated with muscular and glandular over-activity. Botulinum toxins act by preventing release of acetylcholine into the neuromuscular junction. While botulinum toxin type A is commonly available, different manufacturers produce specific products, which are not directly interchangeable and should not be considered as generically equivalent formulations. Type B is also available in the market. Each formulation of botulinum toxin is unique with distinct dosing, efficacy and safety profiles for each use to which it is applied. Botulinum toxin type A is the treatment of choice based on its depth of evidence in dystonias and most other conditions. Botulinum toxin type A is established as useful in the management of spasticity, tremors, headache prophylaxis and several other neurological conditions. Active research is underway to determine the parameters for which the type B toxin can be used in these conditions, as covered in this review. Botulinum toxin use has spread to several fields of medicine.Introduction “All things are poisons, and there is nothing that is harmless; the dose alone decides that something is a poison.” -Paracelsus (1493-1541) Though botulinum toxin is considered to be one of the most toxic substances in nature, commercial preparations have been established through clinical research for wide application in the treatment of several conditions. Since its introduction for treatment of strabismus and focal dystonias in the 1970s, the use of botulinum toxin type A (BoNT/A) has now extended to spasticity, inappropriate body sphincter contraction, eye movement disorders, hyperkinetic movement disorders, autonomic disturbances, cosmetology and pain syndromes. Botulinum toxin type A has several advantages: relatively rare systemic side effects, lack of tissue destruction, graded therapeutic response by dosage adjustment and, above all, high patient acceptance. Botulinum toxin type B (BoNT/B) and BoNT/A (China) are also discussed. Herein, we review the essential aspects of the toxin preparations, their modes of action and therapeutic uses which have been clinically established for each of these at this time. This review was written by selecting key articles written in English after searching the PubMed for literature on “botulinum toxin, pharmacology and medical use”. History Justinus Kerner, a German physician, first described botulism in 1822 in a disorder he called sausage poisoning, for the food that was the source of the epidemic. Sausage in Latin is Botulus. He concluded that there was a poison causing the disease and speculated that the toxin could have a therapeutic role in proper amounts. Emile Pierre Marie van Ermengem, a student of Koch, associated Clostridium botulinum with causation of botulism in 1895. Dr. Edward Schantz prepared crystalline forms of BoNT/A toxin during World War II. In 1981, Dr. Alan B. Scott, an ophthalmologist, first used BoNT/A in clinical practice for strabismus.[1] Subsequently, in the 1980s, BoNT/A was used for blepharospasm and other focal dystonias. Today, it is used in many fields of medicine and approximately 1000 papers can be located on its therapeutic use in electronic databases such as Medline. The United States Food and Drug Administration approved BoNT/A (BOTOX®, Allergan, Inc.) in the management of strabismus, blepharospasm and related facial spasms in 1989 and cervical dystonias in 2000. Botulinum toxin type B first became available commercially in the USA in 2000, and was approved for cervical dystonia, but not for blepharospasm or strabismus. Botulinum toxin A is manufactured under the trade name BOTOX® (Allergan, Inc.) in the United States (marketed as Oculinum® prior to 1992) and DYSPORT® (Ipsen, Inc.) in Europe. In the last few years, BoNT/A is also being produced in China. The Chinese toxin (Lanzhou Biological Products Institute, China) is recently being marketed in India as BTX-A.[2] Botulinum toxin B is available in the U.S. as MYOBLOC® and in Europe as NEUROBLOC®.[1],[2],[3]Structure and Mechanism of Action Botulinum toxins are exotoxins produced by Clostridium botulinum, an anaerobic gram positive sporulating organism. Different serotypes produce different toxins. Botulinum toxin is the most potent toxic substance in nature. Biological activity of the toxin is measured in mouse units, mouse LD50 or simply a 'unit', which is defined as the amount of toxin required to kill 50% of a group of Swiss-Webster mice, after intraperitoneal injection.[1],[4],[5] While LD50 calculations for humans are projections from primate data, 2700-3000 mouse units is the dose usually cited as the LD50 for a 70 kilogram human. For BOTOX® (Allergan, Inc.) 5 nanograms is 100 units, and 135-150 nanograms would be a lethal dose (27-30 vials injected intravenously). Assuming that 10-20 micrograms is the lethal dose orally, 60-120 kilos would be the LD[50] for the human population. While the raw toxin has potential as a biological weapon, hundreds of thousands of vials of the pharmaceutical product would have to be obtained to create a real threat. There are seven serotypes of botulinum toxins, types A-G.[1],[2],[3],[4] Botulism is caused by serotypes A,B,E,F and potentially G. Each botulinum toxin contains a unique zinc-dependent endopeptidase (50 Kilodaltons), the light chain, which is bound to a heavy chain (100 Kilodaltons). A disulfide bond, in complex with hemagglutinin and nontoxin-nonhemagglutinin proteins, holds the heavy and light chains together.[5],[6] Different preparations have different total weights of these complexes, ranging from 300-900 Kilodaltons. The total complex weight may be a factor determining diffusion of the toxin from the site where it is injected. The heavy chain binds to acceptor proteins near the synaptic membrane and subsequently, the light chain enters into the cell and cleaves a specific protein at a specific site. The class of proteins attacked are all part of the Soluble NSF(N-ethyl maleimide-sensitive factor)-Attachment protein REceptor (SNARE) complex [Table - 1] that are involved in exocytosis of acetylcholine vesicles located in the peripheral motor neurons, the primary site of action. Thus, the toxins prevent release of acetylcholine into the synaptic cleft and reduce muscular or glandular activity.[5] With time, nerve sprouting occurs and new neuromuscular junctions are formed. Also, the intoxicated neuron gets reactivated after a period of time specific to each serotype. As a result, the neuron returns to the previous clinical state. Hence the effects of botulinum toxin are fully reversible.[1] When injected, the various preparations of BoNT produce local, temporary and reversible cholinergic chemodenervation of muscles and glands.[5] Botulinum toxin A is preferred because of its long duration of action and ease of production.[1] In addition to chemodenervation, BoNT/A has also been shown to modify the sensory feedback loop to the central nervous system through effects on the muscle spindle and has anti-nociceptive effects in experimental models.[5] Immune responses to BoNT/A and presumably other BoNT preparations can be minimized by using the least required dose and avoiding frequent repeat injections.[1] Current labeling in most countries suggest 12-week separation between doses of BoNT. During manufacturing, BoNT is produced from an anaerobic culture of a specific Clostridium botulinum strain. Adding either sodium chloride (BOTOX®,Allergan, Inc.) or lactose (DYSPORT®, Ipsen, Inc.) protects the steric conformation of BoNT.[1] Human serum albumin is added to prevent loss from surface adsorption. Finally, the toxin is dried either with freezing (DYSPORT®, Ipsen, Inc.) or without freezing (BOTOX®, Allergan, Inc.). Numerous factors influence the clinical potency of the preparation and hence, units of products are not clinically equivalent or interchangeable. Comparative studies between other BoNT/A preparations have not yet been published. A recent study comparing the Chinese Botulinum toxin, available in India as BTX-A®, and BOTOX® shows that both preparations are safe and effective treatments in focal dystonia and various “muscle spasms”. The authors conclude that the Chinese preparation is a little less powerful but much cheaper than BOTOX®.[2] BoNT/B is stable in solution at an acidic pH and is not dried, but is available as a solution containing 5000 units per mL. There is overfill in the MYOBLOC® vials which requires the user to be aware of this relationship of dose to volume for patient injections and for sterile dilutions from the original vial.[7] MYOBLOC®, while nearly equipotent to type A toxin in mice, is less potent in humans than the type A toxins. Doses for MYOBLOC® in cervical dystonia range from 2500-20,000 units. Label instructions or published literature on dosing should be carefully followed for all botulinum preparations, as significant differences exist in their formulations and relative biological effects. Doses given in this paper are for BOTOX® units.[1] Clinical effect of the serotype A and B toxins begins within 24-48 hours, peaks at 2-3 weeks and lasts for 3-4 months.[1],[4],[5] Therapeutic window of a muscle refers to the suitability of a target muscle for BoNT therapy. Botulinum toxin reduces both voluntary and dystonic strength of a muscle. Functional impairment can be avoided by reducing the voluntary strength within the range of its reserve strength. Thus reserve strength of the muscle determines therapeutic window. Finger flexors and extensors and muscles of the lower half of the face have a narrow therapeutic window and hence have higher chances of functional impairment when injected. Orbicularis oculi muscle has wider therapeutic window.[1] Side effects Reduction of physiological strength is an obligatory side effect, yet, is uncommon due to a wide therapeutic window and presence of agonist muscles. This side effect is not seen for glandular tissue.[1] Side effects can either be local transient weakness due to spread to adjacent muscles or systemic spread of unbound BoNT. Systemic spread of botulinum toxins is not expected to result in clinical effects and for type A toxin, is often seen at the level of single fiber EMG studies as jitter in distant muscles. BoNT/B does however produce dry mouth from distal injections and may be due to either more easy systemic absorption or higher affinity for autonomic nerve endings. Usually less than 5% is absorbed and, when BoNT is used in therapeutic doses, manifestations of systemic spread are rare.[1] The non-toxin proteins in the injections can occasionally cause flu-like symptoms. [1] Autonomic side effects probably occur more often with BoNT type B.[8] Action of all BoNTs are believed to be enhanced by aminoglycoside antibiotics.[1] Calcium antagonists may inactivate BoNT. Botulinum toxin should be avoided in pregnancy, in patients with neuromuscular transmission disorders and in impaired hemostasis.[1]Treatment failure Treatment failure can be either primary, where failure occurs in a BoNT-naïve patient, or secondary, where failure occurs after an initial successful use.[1] Treatment failure may result from misplaced toxin, sub-optimal dosing, or administration of toxin that has been inactivated by improper storage or handling. Antibodies to the toxin are presumed to be responsible for most remaining cases of resistance. Treatment failure for antigenicity is assessed when there is either absent or reduced response to BoNT. It is assessed clinically using the Frontalis type A antibody test (FTAT) wherein 15-20 U of BoNT/A are injected into two sites of the muscle and ability to raise the brow at 2 weeks is studied. If eyebrows can be raised, it indicates resistance.[4] Persistence of motor activity with ability to raise the eyebrow during electromyography (EMG) of injected muscles gives electrophysiological evidence of resistance. Antibodies are also detectable using ELISA, sphere-linked immunodiagnostic assay, western blot assay and combined fluorescein- and enzyme-linked assays.[1],[4],[6] Unfortunately, correlation between clinical resistance and detection of antibodies by assays, especially ELISA, has not been established.[6] Mouse neutralization assay /mouse protection assay is considered the gold-standard assay, whereby injected mice will not die if antibodies are present in the test serum, though the meaning of the test in clinical practice is controversial. Early reports indicated that neutralizing antibodies occurred in 3-10% of cervical dystonia patients treated with BoNT/A. The more recent preparations (available after 1997) have lower protein content, eg. currently available BOTOX® has 4-5 nanograms of neurotoxin complex per 100 units. In a recent study of 130 patients treated for cervical dystonia, 42 were treated with the original preparation (used before 1998) of BOTOX® and 119 were treated with the more purified form used currently. Blocking antibodies were not detected in any of the 119 patients treated exclusively with currently used more purified BOTOX®. The authors conclude that the currently used BOTOX® does not produce neutralizing antibodies possibly due to lower protein load.[9] Patients with resistance to BoNT/A may benefit from botulinum toxins B or F (commercially BoNT/F is not available presently), as their immunogenicity profiles are different.[1] Indications for Botulinum Toxin in Neurology The use of botulinum toxin has spread to several areas of neurology [Table - 2]. The dosages given below are for BOTOX®. 1. Dystonia a. Benign Essential Blepharospasm: Dystonic hyperactivity in the orbicularis oculi muscles causes blepharospasm. Botulinum toxin is the treatment of choice. Orbicularis oculi, corrugator supercilii and procerus are targeted; 25 U are generally used for each side. Good results are attributed to large therapeutic window of injected muscles, easy accessibility and distinctness from adjacent muscles. Complications, namely ptosis, dryness of eyes, lateral rectus palsy, facial muscle paralysis and hematoma formation, are transient and reversible.[1],[3],[4] Considerable improvement occurs in the quality of life measures in patients with blepharospasm.[10] b. Meige's syndrome: Patients have dystonia of both upper and lower halves of face. The lower face muscles have a very narrow therapeutic window and thus, have substantially higher chances of functional impairment. The dose used varies between 50 to 100 units. c. Oromandibular Dystonia: In jaw closure dystonia, masseters are targeted bilaterally and 30U of BoNT/A are commonly used for each side. In jaw opening dystonia, lateral pterygoids together with anterior belly of omohyoid are targeted but the response is variable. It is advisable to avoid injecting tongue muscles in lingual dystonia as a weak tongue can choke a patient, requiring intubation.[1],[4] Oromandibular dystonias are difficult to treat without causing dysphagia and should only be done by well-trained and experienced clinicians with adequate experience in use of neurotoxins. d. Cervical dystonias: Botulinum toxin is the treatment of choice for cervical dystonias and they significantly improve the quality of life measures.[1],[4],[11] Identification of the muscles responsible for torticollis, laterocollis, anterocollis and retrocollis is essential. Muscles are targeted specifically after observing the pattern of shift, tilt and rotation of the neck and through EMG assessment. Approximately 20-60 U are needed for a muscle. Anterocollis with head protrusion has a poor response. Side effects include reduced head control and dysphagia. Injections into the sternocleidomastoid and scalenes have a higher risk of dysphagia. Dysphagia can be minimized by avoiding bilateral sternocleidomastoid injections, targeting its insertion and ensuring that the muscle bulk is not penetrated. Patients in whom dysphagia might pose increased risk for aspiration pneumonia should be carefully assessed prior to injection. The effect of injections lasts for around 3-4 months. e. Pharyngolaryngeal dystonias: Botulinum toxin therapy is the treatment of choice for both abductor and adductor forms of pharyngolaryngeal dystonias. Amongst all the indications for BoNT/A therapy, spasmodic dysphonia shows the highest success rate.[1] Botulinum toxin type A is injected either per orally under laryngoscopic guidance or transcutaneously through the cricothyroid membrane under EMG guidance.[1],[4] The vocalis muscle is targeted in the adductor form and posterior cricoarytenoid muscle in the abductor form. Approximately 2.5-10 U are used and the effect begins within 2-3 days and lasts for 2-9 months. Complications include transient dysphagia, weak cough, hoarseness and hypophonia. Dyspnea and stridor can occur after treating the abductor form.[1],[4] Quality of life measures improve significantly after BoNT/A injections.[12] f. Writer's cramp and occupational cramps: Dystonic hyperactivity of forearm, hand and, occasionally, proximal arm muscles while writing occurs in writer's cramp. It is the most common occupational cramp. Response to BoNT/A is better if dystonia is limited to isolated muscles and if the initial hyperactive muscle trigger can be identified. Limitations to therapy include narrow therapeutic window of the wrist and finger flexors, large requirement for BoNT/A due to large number of muscles involved and difficulty to distinguish dystonic action from physiologic and compensatory action.[1],[4] g. Non-action induced limb dystonias: Botulinum toxin type A is useful in pain reduction and improvement in function.[1] 2. Spasticity
3. Hemifacial spasms
4. Exocrine gland hyperactivity b. Relative sialorrhoea: Botulinum toxin type A injection into the parotid gland is effective for controlling drooling in conditions such as Parkinson's disease, motor neuron disease and bulbar/pseudobulbar palsy without causing xerostomia.[1] c. Frey's syndrome: Areas of skin are targeted that show gustatory sweating due to aberrant innervation of facial nerve secretomotor fibers to sweat glands following parotidectomy.[1] d. Crocodile tears syndrome: Lacrimal glands are targeted in gustatory lacrimation due to aberrant innervation of facial nerve secretomotor fibers.[1]
5. Tremors 6. Headache- prophylaxis 7. Other pain syndromes 8. Urinary bladder dysfunction b. Detrusor hyperreflexia: Injection of BoNT/A into the detrusor muscle of the bladder under cystoscopic guidance leads to reduction in hyperreflexia.[1],[27]
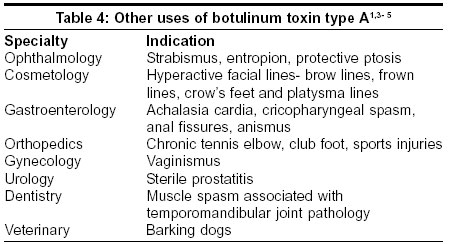
9. Other neurological conditions Other uses of botulinum toxin therapy. [Table - 4] gives an account of the uses of botulinum toxin type A in other fields of medicine and surgery. Botulinum Toxin in India Botulinum toxin type A is available in India as BOTOX® (Allergan, Inc.) and DYSPORT® (Ipsen, Inc.). Recently, the Chinese toxin too has been introduced into the market. Injecting BoNT/A needs training and practice. Most major cities in the country have neurologists capable of injecting BoNT. The cost of treatment with BoNT is expensive as medical insurance is almost non-existent in India. Health insurance covers only 3 per cent of the population. Mediclaim, a state-owned insurance company, covers about 2.5 million Indians and the Employees State Insurance or the Central Government Health Schemes cover another 3 million[28] and patients can obtain the toxin through these schemes. Nevertheless, the cost-benefit ratio is still good and affordable for patients with hemifacial spasm, blepharospasm, occupational cramps and spasmodic dysphonia.Newer directions Research is ongoing to determine newer applications and molecules of botulinum toxin. In clinical trials, botulinum toxin types E and F have shorter duration of action and the latter has been used to treat patients with antibodies or clinical resistance to type A toxin. Botulinum toxin type C may have properties similar to type A but has not come to full-scale trials. The efficacy of toxin fragments is being studied and the deactivated heavy chain is being studied as a carrier of other active substances to the nerve ending.[3],[29] Short acting derivatives are being synthesized for application in sports injuries while preparations are being synthesized that have longer duration by blocking reactivation.[3],[5],[29] Drug delivery using pressure guns is being studied for use in hyperhidrosis to avoid pain. Botulinum toxin type A has become established as a therapeutic tool in a wide range of medical and surgical conditions. It is being explored as an analgesic/anti-inflammatory agent. Judicious use of botulinum toxin will ensure that it continues to be an important therapeutic option and improves the quality of life of patients.References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=455;epage=460;aulast=Muthane The following images related to this document are available:Photo images[ni03150t3.jpg] [ni03150t2.jpg] [ni03150t4.jpg] [ni03150t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}