 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
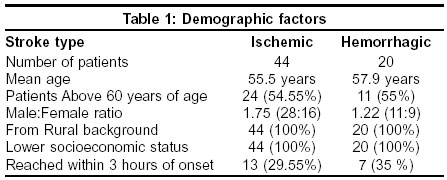
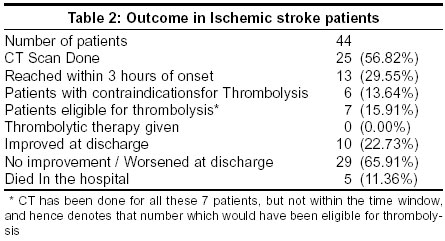
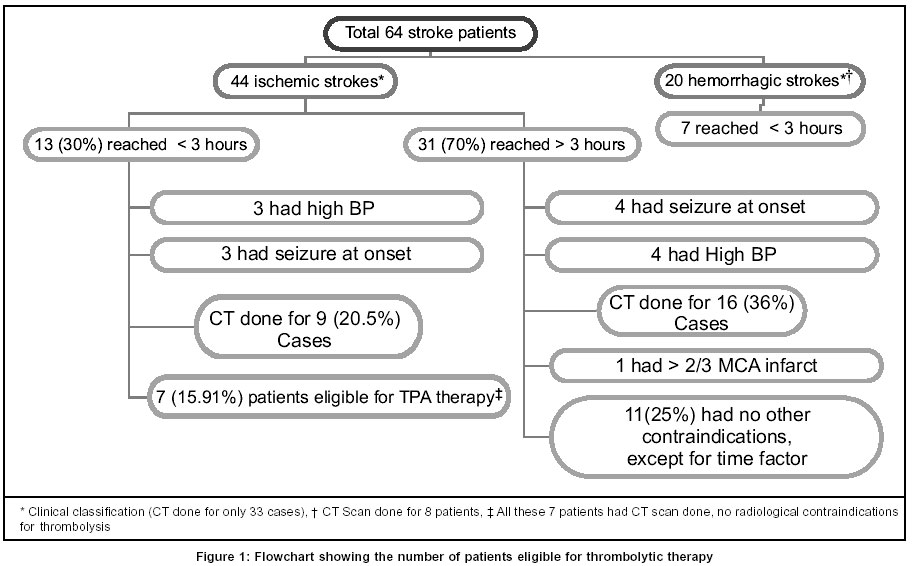
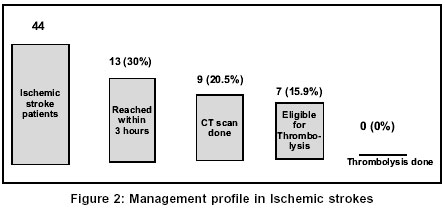
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 470-473 Original Article Feasibility of acute thrombolytic therapy for stroke Nandigam K, Narayan SK, Elangovan S, Dutta TK, Sethuraman KR, Das AK Department of Neurology, Radiodiagnosis and Medicine, Jawaharlal Institute of Post Graduate Medical Education and Research, Pondicherry Code Number: ni03153 Abstract Background: Thrombolysis is an expensive medical intervention for ischemic stroke and hence there is a need to study the feasibility of thrombolysis in rural India. Aims: To asses the feasibility and limitations of providing thrombolytic therapy to acute ischemic stroke patients in a rural Indian set-up. Material and Methods: The first 64 consecutive patients registered under the Acute Stroke Registry in a university referral hospital with a rural catchment area were studied as per a detailed protocol and questionnaire. Results: Of the 64 patients 44 were ischemic strokes, and 20 were hemorrhagic. Thirteen (29.55%) patients with ischemic stroke reached a center with CT scan facility within 3 hours, of whom only 7 (15.91%) were eligible to receive thrombolytic therapy as per the existing clinical and radiological criteria, but none received the therapy. Of the remaining 31 (70.45%) who arrived late, 11 (25%) had no clinical and radiological contraindications for thrombolysis, except the time factor. All the patients belonged to a low socioeconomic status and a rural background. Conclusion: Though a large proportion of ischemic stroke patients were eligible to receive thrombolytic therapy, the majority could not reach a center with adequate facilities within the recommended time window. More alarmingly, even for those patients who reached within the time window, no significant attempt was made to initiate thrombolysis. These data call not only for attention to improve existing patient transport facilities, but also for improving the awareness of efficacy and therapeutic window of thrombolysis in stroke, among the public as well as primary care doctors.Introduction The management of acute strokes continues to be challenging in the new millennium. Thrombolytic agents can be used to re-canalize occluded arteries in selected patients with acute ischemic stroke. Administration of recombinant tissue plasminogen activator (r-tPA) intravenously within 3 hours of stroke onset has been found to be associated with a favorable outcome.[1],[2] The beneficial effect of r-tPA was consistently present in all ischemic stroke subtypes.[3] However, thrombolytic therapy for acute stroke is a complex issue, balancing the benefit of the reversal of ischemia against the risk of symptomatic brain hemorrhage. Intracranial hemorrhage is a major life-threatening complication of thrombolytics.[4],[5] A technically adequate head CT scan is required prior to the administration of thrombolytic therapy to exclude brain hemorrhage and non-ischemic diagnoses. The baseline CT scan is also sensitive for the detection of early signs of cerebral infarction.[6],[7] Patients with early radiographic evidence of major cerebral infarction defined as the presence of mass effect or ischemic hypodensity involving greater than one-third of the middle cerebral artery territory are at substantially greater risk for developing symptomatic intracranial hemorrhage following thrombolytic therapy and have been excluded from several large randomized trials such as ECASS II and ATLANTIS.[8],[9],[10] A recent analysis of baseline CT scans from the NINDS rt-PA Stroke Trial suggested that patients treated with rt-PA within 3 hours of stroke onset had improved clinical outcomes as compared to placebo-treated patients whether or not early ischemic changes could be detected on the baseline CTscan.[11] There are various issues underlying acute stroke therapy, the world over. Some of these issues include poorly informed public, too slow response time, too late presentation, and ill-prepared hospitals. These are surprisingly common to both developed and developing nations, mostly because of the relatively recent therapeutic success of the acute stroke therapy trials.[12],[13],[14] Since the major part of India has a rural background, and since this is a common factor for the rest of the developing world as well, it is extremely important to study these factors to face the challenges in setting up a system for acute stroke care for the world at large. The referral university hospital in which this study was done is in a unique position in that it provides adequate facilities for the intensive care of patients and has its major catchment population from a rural background. The aim of the study was to determine the feasibility and limitation factors of providing thrombolytic therapy for acute ischemic stroke, for a rural population. Material and Methods This is a tertiary hospital-based, descriptive study of acute stroke patients admitted through the emergency medical services. Adult stroke patients who sought emergency medical services were registered under the Acute Stroke Registry during Jun-Aug 2002. All these patients were from rural Pondicherry and the neighboring districts of Tamil Nadu. Detailed history, general, physical and neurological examination and routine investigations including CT scan brain were performed as early as possible. A physician and neurologist verified the neurological status and diagnosis in each case. Special emphasis was laid on history for relevant data such as time to reach a doctor, time to reach a center with facilities for thrombolytic therapy, and time for CT head. Ethical clearance was obtained from the local review board and the research council. Informed consent was taken from the subjects to be included in the study.Results Of the total of 64 patients studied, 44 (68.75%) were ischemic strokes and 20 (31.25%) hemorrhagic strokes [Table - 1]. The diagnosis was confirmed radiologically (CT scan) in only 33 patients. In the remaining 31 patients the stroke subtype diagnosis was based purely on the clinical data. Each case was examined and the diagnosis verified by a physician and a neurologist. The mean age was 56.25 years and 35 (55%) patients were above the age of 60 years. The male to female ratio was 1.56:1. Thirteen (29.55%) patients with ischemic stroke and 7 (35%) with hemorrhagic stroke reached the referral university hospital within 3 hours of onset of acute neurological deficits. Nine (20.45%) of the 13 (29.55%) patients with clinical diagnosis of ischemic stroke who arrived at the emergency department within 3 hours of onset of stroke had CT scan brain. Of these 13 patients, 6 patients had one of the exclusion criteria,[15] 3 had seizures at the onset and in 3 the blood pressure (BP) readings were above 180/100 mm Hg. The remaining 7 (15.9%) patients would have satisfied all the clinical and radiological criteria to receive thrombolytic therapy, had the CT scan been completed within the prescribed time window [Table - 2]. Among the 31 (70.45%) patients with clinically diagnosed ischemic stroke who reached the hospital after the window period, 9 had contraindications for thrombolytic therapy. They included 4 patients with BP readings greater than 185 / 110 mm Hg, 4 patients with seizures at the onset of symptoms, and 1 patient with CT evidence of infarction greater than two-thirds of the middle cerebral artery (MCA) territory. CT head was done in 16 (36.36%) of these 31 patients including the 5 aforementioned patients with contraindications for thrombolysis. There were no other clinical and radiological contraindications for thrombolytic therapy in the remaining 11 (25.0%) patients, had their investigations been completed within 3 hours of stroke onset. Nineteen patients had sudden onset of symptoms either during the late hours of night or early in the morning, which included 15 (34.09%) ischemic stroke patients. Of these, only 3 (6.81%) patients could reach the hospital in less than 3 hours. All the patients were from a rural background, and all belonged to a lower socioeconomic status. Thirteen (20.31% of all stroke patients) were referred by a primary care physician, of whom, only 3 (4.68% of all stroke patients) reached the tertiary care center within 3 hours of onset of symptoms, whereas 51(79.67% of all stroke patients) reached the tertiary care center directly [Figure - 1]. None of the 7 (15.91%) eligible patients with ischemic stroke received thrombolytic therapy [Figure - 2]. The non-availability of an emergency CT scan round the clock was an important factor, which contributed to the apathy towards rt-PA therapy. The cost of rt-PA was another important hindrance, as most of the patients belonged to a lower socioeconomic status and found it absolutely difficult to afford the expenditure involved in thrombolytic therapy. Twenty (31.25%) of the 64 patients with stroke presented at a time beyond the usual working hours of the hospital, of whom 9 (14.06% of all stroke patients) presented within 3 hours of stroke onset, for whom radiological confirmation of the diagnosis was considerably delayed, and rendered them out of consideration for thrombolytic therapy. Due to poor socioeconomic status, most of the patients had to depend on the time-dependent public transport system to reach hospitals. Most of these patients were essentially not aware of the importance of the time factor in stroke management. Discussion This study clearly suggests that there are many hurdles in delivering thrombolytic therapy to eligible patients with acute ischemic stroke in rural India. Lack of public awareness, poor health care delivery systems, and non-affordability of treatment costs were the main factors. Health care delivery policy-makers have to seriously ponder on what measures can be taken to provide the drug to such patients or to find ways to meet the expenditure.[12],[13],[14] Emergency medical service systems should implement a pre-hospital stroke protocol to evaluate and rapidly identify patients who may benefit from thrombolytic therapy, similar to the protocol for chest pain.[13],[14] Stroke patients presenting within 3 hours should be triaged on an emergent basis with an urgency similar to acute ST-elevation in myocardial infarction. The use of an acute stroke care team, including physicians, neurologists, nurses, radiology staff and pharmacists, is an effective way to coordinate initial evaluation and treatment. The round-the-clock availability of CT scanning in the emergency medicine department has to be ensured in district hospital level onwards. Availability of a technician well versed with operating a CT scan machine, round-the-clock, will suffice, without the need for a radiologist, as physicians in the emergency medicine department will be capable of distinguishing an ischemic infarct from an intracranial hemorrhage and they can also be trained to pick up early radiological signs of an evolving infarct in CT images. Mechanisms are also to be worked out to readily make available the only proven drug for acute stroke therapy, i.e., TPA, at the tertiary care centers and district headquarter hospitals, despite the current high cost of the drug. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=470;epage=473;aulast=Nandigam The following images related to this document are available:Photo images[ni03153t2.jpg] [ni03153t1.jpg] [ni03153f2.jpg] [ni03153f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}