 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
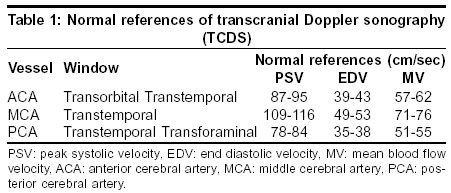
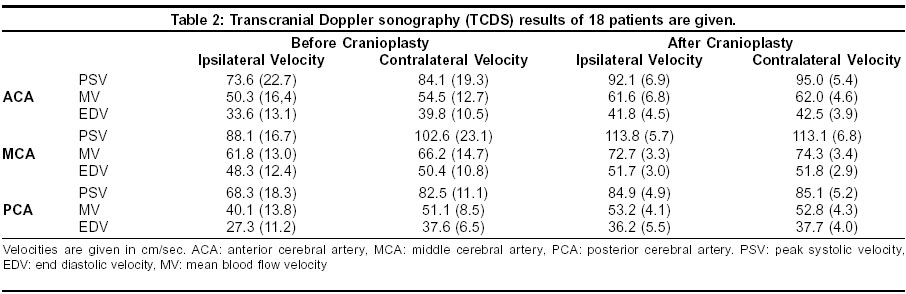
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 479-481 Original Article The effect of cranioplasty on cerebral hemodynamics: Evaluation with transcranial doppler sonography Erdogan E, Düz B, Kocaoglu M, Izci Y, Sirin S, Timurkaynak E Gulhane Military Medical Academy, Department of Neurosurgery, Ankara Code Number: ni03155 Abstract Background: The purpose of cranioplasty is not only cosmetic repair but also neurological improvement. The effect of cranioplasty on the cerebral hemodynamics flow has not been investigated by ultrasonographic techniques. Aims: To investigate changes of cerebral hemodynamics after cranioplasty in patients with cranial defect using transcranial Doppler sonography (TCDS). Setting: The Departments of Neurosurgery and Radiology of a university hospital. Design: A prospective clinical study. Material and Methods: We prospectively examined the cerebral hemodynamics with TCDS pre- and postoperatively in 18 patients with cranial defect who underwent cranioplasty. All postoperative studies were done between the 7th and 15th day after cranioplasty. The anterior cerebral artery was examined through the transtemporal and transorbital windows, the middle cerebral artery through the transtemporal window, and the posterior cerebral artery through the transforaminal window. Bilaterally, the peak systolic, end diastolic and mean blood flow velocities of these arteries were measured. Statistical Analysis: Wilcoxon matched-pairs signed-ranks test. Results: Before cranioplasty all the velocities ipsilateral to the cranial defect were significantly low, while in the contralateral side they were near normal. Ipsilateral low cerebral blood flows increased and reached normal levels (P<0.05) after cranioplasty. During the follow-up, neurological improvement was observed. Conclusion: Cranioplasty is carried out not only for preserving normal appearances and physical barrier but also for neurological improvement. This should be explained by the normalization of cerebral hemodynamics.Introduction It is well known that decompressive craniectomy is indicated for cranial gunshot wounds and other trauma. Many patients with severe gunshot wounds have larger cranial defects and neurological deficits.[1] There is little information on the relationship among cranial bone defect, cerebral hemodynamics and neurological improvement.[2] Yoshida et al studied cerebral blood flow and metabolism in 7 patients after cranioplasty by 133Xe computed tomography and [31]P magnetic resonance spectroscopy and demonstrated the increase in cerebral blood flow and the decrease in neurological deficits.[3] The main indications of cranioplasty include cosmetic repair and restoration of cerebral protection. The objective of this study was to investigate the effect of cranioplasty on cerebral hemodynamics in patients with cranial defects using pre and postoperative transcranial Doppler sonography (TCDS). Material and Methods Eighteen patients (17 males and 1 female) who presented at the Gulhane Military Medical Academy Department of Neurosurgery with cranial gunshot wounds or other trauma between 1995 and 1999 were included in the study. Cases with cerebrovascular, cardiovascular or peripheral vascular disorders accompanying primary pathology were excluded from this study. The etiology of the cranial defect was gunshot wounds in 10 patients and other trauma in 8 patients. Parietal and frontal bone defects were observed in 14 patients. The findings on neurological examination were hemiparesis in 9 patients, monoparesis in 2 patients, paraparesis in 1 patient, normal in 6 patients and “syndrome of trephined” in 18 patients. Cranial computed tomography (CT) scanning was performed in all patients. The CT findings were encephalomalacia in 15 cases, foreign body in 6 cases, dural thickening in 2 cases and normal in 3 cases. The median time before cranioplasty was 12 months (ranging between 9 and 22). Methylmethacrylate (Codman cranioplastic kit®, USA) was used in 17 patients and autograft was used in 1 patient. All patients were evaluated by TCDS before and after cranioplasty. The factors that could affect cerebral hemodynamics during TCDS such as fatigue, hunger, alteration of arterial blood pressure, audiovisual stimulation and emotional alterations were eliminated. All postoperative studies were performed within 7 to 15 days after cranioplasty. The patients were examined using Acuson 128 XP/10 computed sonography and 2.5 MHz 900 sector viewing V219 transducer (USA) though 3 windows-transorbital, transtemporal and transforaminal (transoccipital). The cranial defect itself was not used as an examination route. The Doppler spectrum of each artery was obtained using 300-600 insonation angle with angle correction. We used the lowest level of sample size and wall filter. Aliasing artifacts were eliminated by optimum baseline correction. After the frozen stable waveform was obtained, peak systolic velocity (PSV), end diastolic velocity (EDV), and mean blood flow velocity (MV) of the middle cerebral artery (MCA), the anterior cerebral artery (ACA) and the posterior cerebral artery (PCA) were calculated by cursor pointing. Means, with standard deviations, of PSV, EDV, and MV in all ipsi- and contralateral MCA, ACA and PCA were calculated. The difference was analyzed by the Wilcoxon matched-pairs signed-rank test. P values lesser than the threshold of 0.05 were considered significant. All procedures to investigate the patients were approved by the ethics committee of the Gulhane Military Medical Academy and written consent for participation in the study was obtained from each patient. At the beginning of the study TCDS was performed on 24 healthy males (mean age 21 years) in order to achieve the normal references of TCDS [Table - 1]. The control group was matched with the study group (18 patients) with regards to gender and age. Results Patients were invited to assess neurological status 1 year after cranioplasty. Fifteen of them accepted, while 3 could not return because of social problems, but they were interviewed by telephone. None of the patients experienced total recovery after cranioplasty. Fourteen of the patients with “syndrome of the trephined” reported that they had improved after cranioplasty. Their main complaints of headache, insomnia, memory disturbance, mental depression and local discomfort on sudden movement had diminished. Hemiparesis improved in 5 patients. Others remained unchanged after cranioplasty. Comparisons of PSV, MV and EDV of the ACA, the MCA and the PCA before and after cranioplasty are given in [Table - 2]. All the velocities ipsilateral to cranial defects before cranioplasty were significantly low, and contralaterally they were near normal. After cranioplasty, the blood flow velocity of the cerebral arteries ipsilateral and contralateral to the cranial defect was increased and reached normal levels. Statistically significant differences between the values before and after cranioplasty were detected in PSV for the ACA (P=0.0002), in MV for the ACA (P=0.0045), in PSV for the PCA (P=0.0014), in MV for the PCA (P=0.0046), and in PSV for the MCA (P=0.0002) on the ipsilateral side. There were statistically significant differences between the values before and after cranioplasty in PSV for the ACA (P=0.0043), in MV for the ACA (P=0.0086), and in MV for the MCA (P=0.0038) on the contralateral side. There were no statistically significant differences between EDV of all arteries on both sides (P=0.2959 for the ACA, P=0.7049 for the MCA, and P=0.9246 for the PCA on the contralateral side, P=0.1020 for the ACA, P=0.3520 for the MCA, and P=0.7564 for the PCA on the ipsilateral side). Discussion The incidence of trauma through wars, traffic accidents, and cerebral gunshot wounds, and multiplying neurosurgical procedures have resulted in an increase in cranial bone defects. In the series of Erdogan et al (2002), 195 (52%) of 374 patients with craniocerebral gunshot wounds had large cranial defects and underwent cranioplasty at least one year after the incident.[1] The universally accepted indications for cranioplasty are cerebral protection and cosmetic repair of the patient. Sometimes cranioplasty should be done to protect the patient from cerebral seizures, to relieve the “syndrome of trephined”, to protect the brain from direct atmospheric pressure, and to correct the shift of central structures. However, these are not generally accepted as an indication for cranioplasty.[2],[4],[5],[6] Neurological recovery after cranioplasty has attracted attention among neurosurgeons in the last two decades. Some reports emphasized unexpected neurological recovery after cranioplasty.[7],[8],[9],[10] The mechanism of neurological recovery after cranioplasty remains unclear to date. Various mechanisms of the relationship between the cranial defect and cranioplasty were suggested and investigated.[3],[8],[9],[10],[11] Restoration of cerebral hemodynamics as an explanation for neurological recovery after cranioplasty was proposed by Richaud et al in 1985.[8] Eight of 15 cases with cranial defect and neurological deficits improved in this study. Hatashita et al studied the effect of craniectomy on the biomechanics of normal brain in animals in 1987.[12] They demonstrated that a large craniectomy causes a decrease of pressure in both the cerebrospinal fluid and the normal brain parenchyma. Suzuki et al investigated the cerebral blood flow with dynamic CT scanning in patients who underwent cranioplasty in 1991.[10] They suggested that an increase in the bilateral cerebral blood flow after cranioplasty might play a role in the patients' neurological recovery. Yoshida et al studied cerebral blood flow and metabolism in 7 patients with stable 133Xe computed tomography and [31]P magnetic resonance spectroscopy and demonstrated the increase of cerebral blood flow and the decrease of neurological deficits in 1996.[3] Winkler et al investigated cerebral blood flow reactivity with TCDS and cerebral glucose metabolism with positron emission tomography in 12 patients and concluded that cranioplasty appears to affect postural blood flow regulation.[2] They also reported no significant difference in resting blood flow velocities but a striking improvement of cerebral vascular reserve capacity ipsilaterally and contralaterally. TCDS is a widely accepted non-invasive method to measure the intracranial arterial perfusion rates in adults and children.[13],[14] Westra et al reported a study on perioperative Doppler sonography in young children undergoing craniosynostosis repair surgery.[15] The advantages of TCDS include low cost, non-invasiveness and lack of radiation. The changes of cerebral hemodynamics could easily be shown by TCDS. In our study the changes in PSV and MV values were statistically significant in the detection of cerebral hemodynamics after cranioplasty but there was no significant change of EDV values, presumably due to stable diastolic cerebral blood flow velocity as a protection mechanism. The comparison of preoperative and postoperative ipsilateral and contralateral PSV, EDV and MV of the MCA, the ACA and the PCA showed that the differences between the study group and the control group were statistically significant (P<0.05). We suggest that every cranial defect allows transmission of direct atmospheric pressure onto the intracranial contents, especially on the blood vessels. Before cranioplasty the whole vascular structure in both hemispheres was affected in the same manner by intracranial pressure through the affected area. When the velocities were compared between the contralateral side and the ipsilateral side after cranioplasty, all the velocities in the MCA, the ACA and the PCA were found elevated after cranioplasty. Conclusion Cranioplasty is carried out not only for preserving normal appearance and physical barrier but also for neurological improvement. TCDS is an effective, non-invasive and inexpensive method of detecting changes of cerebral hemodynamics. Neurological improvement after cranioplasty can be explained by improvement of cerebral hemodynamics.References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=479;epage=481;aulast=Erdogan The following images related to this document are available:Photo images[ni03155t2.jpg] [ni03155t1.jpg] |
| |||||||||

{kind=link}
{kind=link}