 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
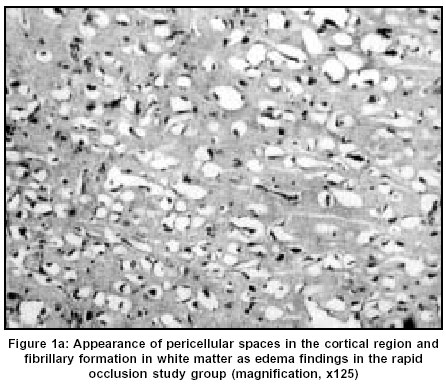
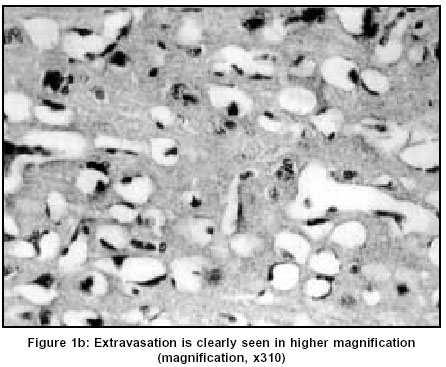
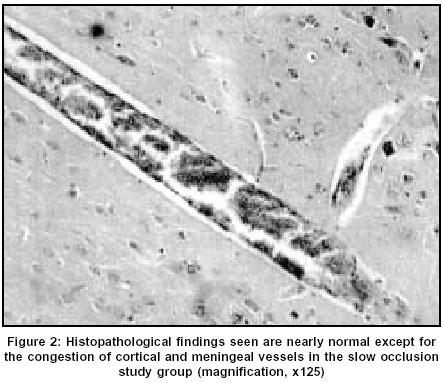
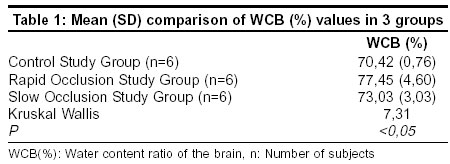
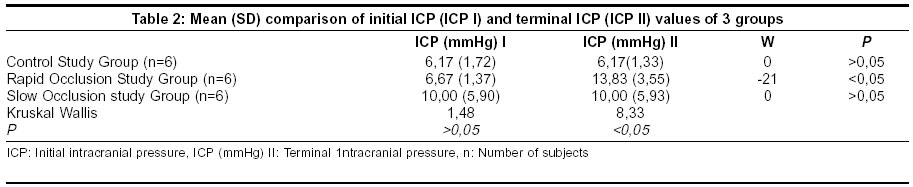
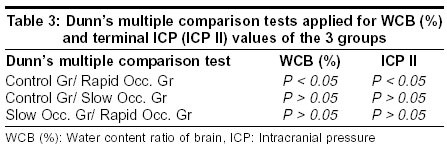
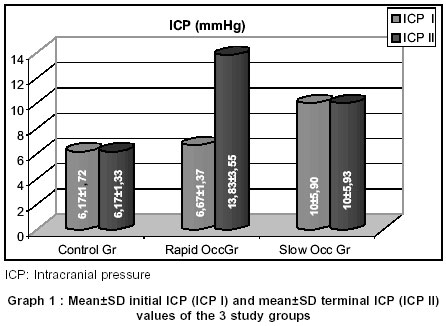
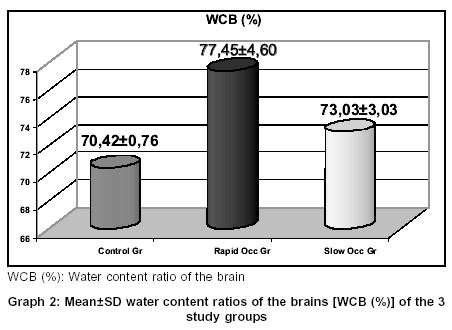
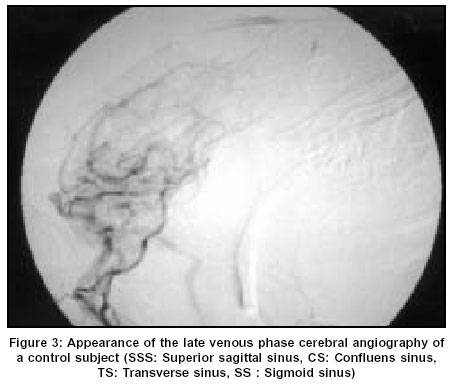
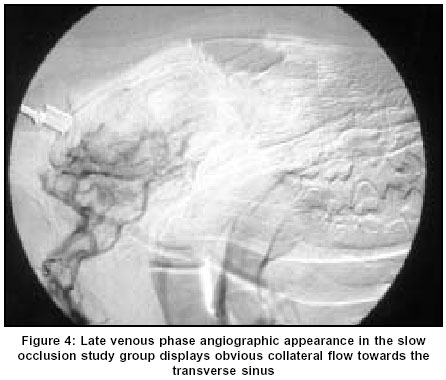
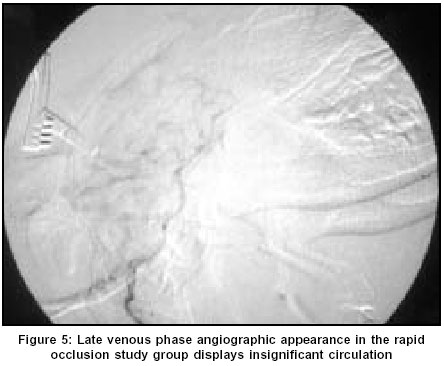
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 482-486 Original Article Experimental study of rapid versus slow sagittal sinus occlusion in dogs Tuzgen S, Canbaz B, Kaya AH, Sanus GZ, Kuday C, Memis M, Oz B Department of Neurosurgery, Cerrahpasa Medical Faculty, University of Istanbul Code Number: ni03156 Abstract Background: Clinical, radiological, postmortem and experimental studies are not enough for the definition of pathophysiological differences between rapid and slow-progressing cerebral venous system obstruction. Aims: An experimental study was conducted to set some physiopathological differences between rapid and slow occlusion of the superior sagittal sinus. Settings and Design: Eighteen dogs categorized into 3 groups were chosen as test subjects. The three groups were the rapid occlusion, slow occlusion and the control study groups and each group had six subjects. Material and Methods: Intracranial pressure values, histopathological findings, and the degree of cerebral edema formation, estimated by measuring the water content ratio of the brain and the angiographic results in the 2 different groups of subjects that underwent rapid and slow superior sagittal sinus obstruction were compared with that of the control subjects. Statistical Analysis: Statistical analysis was performed using GraphPad Prisma V.3 statistical software. Variables of the 3 groups were compared using non-parametric Kruskal Wallis ANOVA test and multiple comparisons were made using Dunn’s multiple test. The comparison of initial and terminal 1ntracranial pressure values obtained before and after the sinus occlusion, was made using the Wilcoxon test. A probabability value of less than 0,05 was regarded as significant. Results and Conclusions: Comparison of the water content ratio of the brain in the 3 groups, the difference between the initial and terminal intracranial pressure values of the rapid occlusion study group, and the difference between the terminal intracranial pressure values of the 3 groups was statistically significant (P<0,05). Dunn’s Multiple Comparison Test yielded significant differences in the water content ratio of the brain and in the intracranial pressure values between the rapid occlusion study group and the control group (P<0,05). Moreover, histopathological and radiological examination disclosed more prominent brain edema findings, and less apparent collateral venous flow in the rapid occlusion study group than in the slow occlusion one. To conclude, the clinical severity of sinus occlusion seems directly related to the quickness of the occlusion and the capacity of the collateral venous system. Introduction Cerebral venous system obstruction leads to parenchymal changes in the brain according to the severity of venous congestion. Etiology, localization and duration of the occlusion are important determinants for the degree of parenchymal changes, and clinical findings change from pseudotumor cerebri to severe venous infarct.[1],[2],[3],[4] Even though obliteration or resection of the dural sinuses and their clinical results are not unusually experienced in some neurosurgical operations, radiological, postmortem and experimental studies are not enough to define the exact pathological differences between rapid and slowly progressing superior sagittal sinus (SSS) obstruction.[4],[5] SSS invasion is usual, especially with parasagittal meningiomas, and morbidity and mortality due to surgical resection would be decreased if the pathophysiology of the occlusion was fully understood. Importantly, although the acute occlusion of the posterior third of the SSS has definite clinical findings,[6] in most of the cases of slow-progressing pathologies such as parasagittal meningiomas, total obliteration of the sinus is without any neurological findings. Studies of experimental dural sinus occlusion[6],[7],[8],[9],[10],[11] reported different results in some respects, probably due to the absence of a standardized experimental model; none of them is a comparative experimental study for rapid and slowly progressing dural sinus occlusion. In this comparative experimental study, intracranial pressure values, histopathological findings, the degree of edema formation and the angiographic results were obtained from 2 different groups of subjects that underwent rapid and slow SSS obstruction, and their results were compared with that of the control subjects. Material and Methods Eighteen healthy street dogs with different genus, 3 to 6 years old, weighing 20 to 25 kg were identified as test subjects. There is a marked similarity of the venous sinus anatomy between dogs and humans. These subjects were taken from the animal dispensary of the municipality and the experiment was performed in the dipsensary clinic. They were categorized into 3 groups, each containing 6 subjects and the groups were named as rapid occlusion study group, slow occlusion study group and control study group respectively. Sedation was achieved by xylazine 0,2 mg/kg (Rompun - Bayer) by intramuscular injection, and 2,5 mg/kg ketamin hydrochloride (Ketalar - Eczacibasi) was used for induction of anesthesia. The ketamin application was repeated as required during the study. The subjects were positioned in sphinx and a 4-cm long median incision was performed in the parieto-occipital region after local application of 50 mg lidocaine subcutaneously. A burr-hole with a 2-cm diameter exposing the confluence sinus and the posterior part of the SSS was achieved for each subject. Epidural sensor Steritek P 1500 (Ladd/ Steritek, Germany) was also applied for intracranial pressure monitoring of each subject. All subjects in the control study group were monitorized for 4 hours. At the 3rd hour, 2 ml of 2% Evans Blue solution was introduced intravenously and the subjects were sacrificed after intravenous potassium chloride application at the end of the monitorization time. In the rapid occlusion study group, falx cerebri was verified first by incising the dura on either side of the SSS, then acute occlusion of the SSS was achieved by a McFadden aneurysm clip. Monitorization time after the obliteration of the sinus was 4 hours and subjects were injected with Evans Blue and sacrificed in the same manner as the control study group. In the slow occlusion study group, SSS occlusion was achieved by a modified Popen clamp rotated once at 15-minute interval, and total occlusion was reached at the end of the first 4-hour monitorization. After total occlusion of the sinus, additional monitorization for 4 hours was also completed. Evans Blue was administered intravenously and the subjects were sacrificed in the same manner as the other groups at the end of the second 4-hour monitorization period. After the brain of the sacrificed subjects had been totally decapitated, extravasation of the Evans Blue was evaluated with 3 coronal cuttings performed on the anterior, middle and posterior part of the brain. A piece of tissue obtained from the posterior part of the brain of each subject was fixed in 10% formaldehyde solution, and histopathological examination of that tissue was achieved with Hematoxylin-Eosin stain. Water content ratio of the brain tissue, WCB (%), was also determined with a piece of white matter (5 to 10 mg) obtained from the posterior part of the brain. After the tissue had been weighted sensitively as a wet tissue weight, it was covered with aliminium foil and kept for 72 hours in an oven at 100 C°, and lastly dry tissue weight was also verified. Water content ratio of the brain tissue was calculated by the formula below: WCB (%) = {[Wet tissue weight (g) - Dry tissue weight (g)] / Wet tissue weight(g)} x 100 For intracranial pressure monitorization, Steritek P 1500 monitor and its epidural sensor (Ladd/ Steritek, Germany) were used in each subject. Digital subtraction angiography was also performed in 1 subject from each of the 3 study groups. The angiographic evaluations were performed at the end of the 4 hours of monitorization in the control study group, at the 4th hour of occlusion in the rapid occlusion study group and at the end of the second 4-hour monitorization in the slow occlusion study group. 4F Pickard catheter (Balt - France) was used in the angiography via the right femoral artery. Lopamidol 300 mg/kg injection was administered and the venous phase in the lateral projection was observed with the rate of 2 scans per second lasting for 1 minute by Philips diagnost 96 DSI. Statistical analysis was performed using GraphPad Prisma V.3 statistical software. The variables of the 3 groups were compared using non-parametric Kruskal Wallis ANOVA test and multiple comparisons were made using Dunn's multiple test. Comparison of the initial and terminal 1ntracranial pressure values was made using the Wilcoxon test. A probability value of less than 0,05 was regarded as significant. Results In the macroscopical examination of the brain tissues, no abnormal finding was observed and there was no extravasation of the injected Evans blue. However, histopathological examination was different in each study group, which showed normal histopathological findings in the control study, subarachnoidal hemorrhage, minimal parenchymal hyperemia, significant edema and slight erythrocyte extravasation in the rapid occlusion study, and neuronal ischemic changes in 3 and slight edema in 4 subjects of the slow occlusion study groups [Figure 1a], [Figure 1b] & [Figure - 2]. None of the subjects revealed thrombus formation in the SSS. Water content ratios of the brain [WCB (%)] obtained from the 3 groups were compared as means±SD [Table - 1] and were statistically significant (KW: 7,31, P<0,05). There was no significant difference between either the control study group and the slow study group or the slow study group and the rapid study group. The difference between the WCB (%) values of the control study group and the rapid study group was statistically significant. The initial intracranial pressure (ICP I) values that were measured at the beginning of the monitorization of the 3 groups, and the terminal intracranial pressure (ICP II) values measured at the end of the total monitorization time of all the groups were also compared as means±SD [Table - 2] and there was statistically significant difference between the initial and the terminal ICP values of the rapid occlusion study group (W: 21, P<0,05). The differences between the initial and the terminal ICP values of the slow occlusion study group and the control study group were found as insignificant. In this same comparison, the difference between the terminal ICP values of the 3 groups were statistically significant (KW : 8,33, P<0,05). When the Dunn's Multiple Comparison Test was applied for WCB (%) and the terminal ICP values of the three study groups [Table - 3], the difference in these two values of the control study group and the rapid occlusion study group was statistically significant (P<0,05). These same results were also illustrated in graphs and the Graph 1 shows mean±SD initial and mean±SD terminal ICP values whereas Graph 2 shows the mean±SD WCB (%) values of the 3 study groups. In the late venous phase of digital substraction angiography, the slow occlusion subjects revealed more obvious filling of the transverse sinus via the posterior anastomotic venous group than the control subjects, whereas this finding was not apparent in the subjects of the rapid occlusion study group [Figure - 3], [Figure - 4] and [Figure - 5]. Discussion Although encountered quite often clinically, the experimental studies relating dural sinus occlusion are not as many as those relating the occlusion of the occlusion of the arterial territory of the central nervous system. In one large autopsy series of 12.500, the incidence of SSS thrombosis was observed as 16.[12] Most of the angiographical results and autopsy findings of the SSS thrombosis were correlated with brain edema formation and high ICP values.[1],[13] Clinical, radiological and experimental studies obviously suggested that acute venous occlusion may lead to increased ICP, alteration of the perfusion pressure of the brain, namely hypoperfusion and lastly, infarction and edema formation.[7],[10],[11] Measuring water content ratio of the brain [WCB (%)] is a method used in experimental studies to asses the severity of brain edema, and previous studies observed an increase in WCB (%) in subjects who underwent SSS occlusion.[6],[7] More interestingly, additional injection of alpha cyanoacrylate or fibrin glue to the occluded sinus in these studies resulted in histopathological findings with regional hemorrhage, macroscopical extravasation of Evans Blue, more significant rise in ICP and water content ratios of the gray and white matters. The previous observation of an increase in the number and volume of the capillary system at the 15th minute of acute sinus occlusion was believed to delay the brain edema formation up to first two hours of occlusion.[8] In another technical report, the infiltrated SSS with basal cell carcinoma was declared as completely excised at 2 cm proximal to the confluence sinus by periodic clipping technique lasting 15 minutes for each 3 cm distance from anterior to posterior, without early and late postoperative morbidity.[14] Additional venous capacity such as collateral venous network possibly plays an important role in determining the severity of the pathophysiological events which occur after the sinus occlusion, and the collateral venous system may have enough time to work more appropriately in slow-progressing sinus occlusion. In our study, angiographically proven collateral circulation in a subject of the slow occlusion study group and not in the rapid occlusion study group was noted as an important finding of the better adaptation of the collateral venous system in slow-progressing SSS occlusion than the rapid progressing one. In our comparative study, the rapid occlusion study group displayed minimal parenchymal hyperemia, slight extravasation of erythrocyte and mild degree of edema formation. On the other hand, in the slow occlusion study group, there were 3 subjects with neuronal ischemic changes, 4 subjects with slight degree of edema formation and 3 subjects with endothelial activation. None of the subjects displayed intraparenchymal or subarachnoidal hemorrhage. These findings showed that histopathological changes were milder in the slow occlusion study group than in the rapid occlusion group. Observation of statistically significant increase of WCB (%) in the rapid occlusion study group was also a valuable finding to disclose the more prominent edematous reaction of the brain to rapid occlusion of the SSS than to slow occlusion of the SSS. Mild brain edema or absence of brain edema in the slow-progressing sinus occlusion study group as compared to the rapid-progressing one may be related to the adaptation of the reserved capillary system to the collateral venous system. It is concluded that in acute sinus occlusion, the time interval is not enough for the collateral venous system to work properly, and it is more likely that the development of venous hypertension, extravasation and venous infarcts will occur. On the other hand, in slowly progressing sinus occlusion, the participation of venous collaterals relieves venous hypertension. The clinical severity of sinus occlusion is directly related to the rapidity of the occlusion and the capacity of the collateral venous system. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=482;epage=486;aulast=Tuzgen The following images related to this document are available:Photo images[ni03156f1a.jpg] [ni03156t1.jpg] [ni03156g1.jpg] [ni03156g2.jpg] [ni03156f1b.jpg] [ni03156f3.jpg] [ni03156t2.jpg] [ni03156f2.jpg] [ni03156t3.jpg] [ni03156f5.jpg] [ni03156f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}