 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
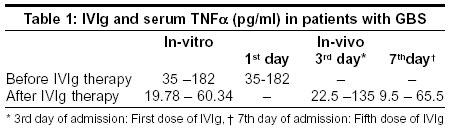
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 487-489 Original Article Intravenous immunoglobulin reduces serum tumor necrosis factor α in patients with Guillain-Barre Syndrome Reuben S, Sumi MG, Mathai A, Nair MD, Radhakrishnan VV Departments of Pathology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram - 695011 Code Number: ni03157 Abstract Background: Tumor necrosis factor a TNF-alpha has a possible role in the pathogenesis of the Guillain-Barre' syndrome (GBS). Aims: To study the effect of intravenous immunoglobulin (IVIg) on serum TNF-alpha concentrations in patients with GBS. Material and Methods: The effect of IVIg on TNF-alpha was evaluated in 36 patients with GBS. Serum TNF-alpha concentration was measured by enzyme-linked immunosorbent assay (ELISA). The sera of 22 (61%) patients with GBS showed elevated concentrations of TNF-alpha (35-182 pg/ml) and these sera were individually incubated in vitro with IVIg (0.25mg/ml) at 37°C for 24 hours. Results: The serum TNF-alpha concentrations in the 22 GBS patients with elevated levels showed a steady decline (60.34-19.78 pg/ml) following incubation with IVIg. These 22 patients also received IVIg therapy, and serum TNF-alpha concentrations showed a significant decline (65.5-9.75 pg/ml) at the end of the therapy. At the time of discharge from the hospital, there was a positive correlation between neurological recovery and decline in TNF-alpha concentrations in these 22 GBS patients. Conclusions: The results of this study indicate that elevated levels of TNF-alpha occur in a proportion of patients with GBS and in these patients elevated serum TNF-alpha levels decline with IVIg therapy.Introduction Guillain-Barre syndrome (GBS) is an acute inflammatory demyelinating polyradiculopathy of undetermined etiology. Currently available evidence suggests that the disease is immunologically mediated and peripheral nerves are essentially involved in this disease. Asbury et al[1] demonstrated lymphocytic infiltration in the peripheral nerves, especially during the active phase of the disease. Immunohistochemical methods revealed that many of these lymphocytes are T cells.[2] The levels of circulating tumor necrosis factor-alpha (TNF-alpha) are also elevated in patients with GBS and are implicated in the pathogenesis of the disease.[3],[4] Activated T lymphocytes and macrophages are the principle source of cytokines, including TNF-alpha-a primary mediator of inflammation. There is evidence that TNF-alpha is capable of inducing selective and specific damage to myelin in vitro.[5] During the past decade, IVIg has emerged as a therapeutic agent in the management of several immunologically mediated demyelinating disorders of the peripheral nervous system, including GBS. Though the precise role of IVIg is undetermined, several immunomodulatory mechanisms of the action of IVIg have been described.[6] Understanding the mechanism of the action of IVIg will not only promote the judicious use of IVIg but also will help in monitoring its dosage in the management of autoimmune demyelinating disorders of the central nervous system. Material and Methods Sree Chitra Tirunal Institute for Medical Sciences and Technology (SCTIMST), Thiruvananthapuram, Kerala State, India, is a major tertiary referral center for neurological diseases. During the year 2000-2001, 36 GBS patients from several hospitals within Kerala state were referred to this hospital for specific management. The clinical history of these patients did not indicate any definite demographic pattern The clinical diagnosis of GBS was based on Asbury's diagnostic criteria.[7] At admission, the patients were classified into clinical stages II-V (Stage II n=8, Stage III n=14, Stage IV n=12, Stage V n=2). TNF-alpha estimation in the sera of patients with GBS was carried out using commercial ELISA kits (Sigma Chemicals, St. Louis, USA). Of the 36 patients, 22 had high serum concentration of TNF-alpha (35-182 pg/ml) and the serum TNF-alpha concentration ranged between 4.4-30 pg/ml in the remaining 14 patients. Patients with high titers were included in the study. Sera from 36 non-GBS patients were selected as disease control, (a) peripheral neuropathy n= 18; (b) myeloradiculopathy n= 5; (c) transverse myelitis n=8; (d) paralytic rabies n=3; (e) chronic inflammatory demyelinating polyneuropathy n= 2. The serum samples from 40 age-matched healthy voluntary blood donors, attending the department of Transfusion Medicine of this institute were collected as healthy controls. At the time of admission, venous blood samples (6-8 ml) from GBS patients and control groups were collected in sterile glass tubes and were allowed to clot spontaneously over one hour. The serum was collected by centrifugation and filtered through 0.22m disposable sterile filter (Millipore) to remove the contaminating particulate material. All the sera samples were collected and frozen at -700C in aliquots until the time of the assay. Repeated thawing and freezing was avoided. Ten thousand Kellikerin units of Proteinase inhibitor aprotinin were added to all the sera samples to prevent protein degradation. The following four variables were used in the in vitro study: (I) 500ml of human TNFa (250 pg/ml) was incubated with 0.25 mg IVIg (Bharat Serum and Vaccine, India), (II) 500 ml sera from controls and each of the 22 GBS patients with high titers of TNF-alpha were individually incubated with 0.25 mg IVIg, (III) 500 ml 0.15M phosphate-buffered- saline (PBS) was incubated with human TNF-alpha standard (250pg/ml), (IV) 500 ml of 0.15M PBS was incubated with 0.25mg/ml IVIg. All the above four variables were incubated under aseptic laboratory conditions (370C for 24 hours) following which they were centrifuged at 5000 rpm for 10 min. TNF-alpha estimations from the supernatant were performed by a sandwich ELISA method, using TNF-alpha immunoassay kits (Sigma). The TNF-alpha immunoassay was performed according to the manufacturer's instructions. Prior to the estimation of serum TNF-alpha concentration in clinical specimens, the immunoassay was standardized with the human TNF-alpha standard. To each well in the ELISA micro titer plate (precoated with mouse monoclonal antibody to human TNF-alpha), 200 ml of human TNF-alpha standard in serial decreasing dilutions (500 - 4.5 pg/ml) was added and incubated for 2 h at room temperature. Following that the plate was thoroughly washed three times with wash buffer. Subsequently, 200ml of TNF-alpha conjugate (polyclonal antibody to TNF-alpha conjugated with horse radish peroxidase) was added to each well and incubated for 2 h at room temperature. The plates were thoroughly washed. A color reaction developed with a substrate containing equal volumes of stabilized hydrogen peroxide and tetra methyl benzidine. The color reaction was stopped after 20 min by the addition of 2N sulphuric acid. The absorbance in each well was measured at 450nm. The absorbance obtained at each dilution of the TNF-alpha standard was plotted and a linear standard graph was obtained. The serum TNF-alpha concentrations in GBS patients, diseased and healthy controls were similarly assayed and the values were measured directly from the standard graph. The lowest detection limit of serum TNF-alpha in this assay was 4.4 pg/ml. All the 22 GBS patients with elevated serum TNF-alpha levels received IVIg (400 mg/kg body weight/day for 5 consecutive days) during their hospital stay. Sera samples were collected before IVIg therapy and also following the first and fifth doses of IVIg (on the third and seventh day following admission). Serum TNF-alpha estimations were performed by a sandwich ELISA, under identical laboratory conditions as described in the in-vitro method. The TNF-alpha values in the GBS and control groups were tabulated. For statistical analysis, Mann-Whitney and student's 't' tests were used to compare the data in the GBS and control groups. Results In the healthy control group and the diseased control group, except in two patients with chronic inflammatory polyneuropathy, the serum TNF-alpha levels were < 4.4 pg/ml. In the two patients with chronic inflammatory polyneuropathy, the serum TNF-alpha concentrations were 25 pg/ml and 30.5 pg/ml respectively. A 'cut-off' level was chosen at 31 pg/ml in the ELISA because at this 'cut-off' it was possible to distinguish GBS patients with elevated TNF-alpha from patients in the diseased control group. Accordingly, 22 out of 36 GBS patients had elevated levels of TNF-alpha concentration (61%) and they ranged between 35-182 pg/ml (P< 0.005). In these 22 GBS patients, there was a positive correlation between the elevated serum TNF-alpha concentration and the disease severity. Patients in clinical stages IV-V had higher serum TNF-alpha concentrations than patients in clinical stages II -III (P<0.05). The serum TNF-alpha concentration in these 22 patients with GBS showed a progressive decline [Table - 1] following a complete course of IVIg therapy (65.5 to 9.75 pg/ml). At the time of discharge from the hospital there was a positive correlation between neurological recovery and the decreasing TNF-alpha concentration in all the 22 GBS patients. Among these 22 GBS patients, 8 patients had antecedent upper respiratory infection and in the remaining 14 patients there were no antecedent events. The serum TNF-alpha concentrations in GBS patients with and without antecedent infection were not statistically significant (P>0.05). The results of the in-vitro studies also indicated a significant reduction in the TNF-alpha concentration following incubation of the sera of GBS patients with IVIg and it ranged between 60.34 - 19.78 pg/ml (P <0.05). Similar results were observed in the in-vitro study, when IVIg was incubated with human TNF-alpha standard and the concentration decreased from 250 to 140.5 pg/ml. The TNF-alpha concentration remained unaltered when human TNF-alpha was incubated with 0.15M PBS. In other words, reduction in the TNF-alpha levels in-vitro was specifically brought by incubation with IVIg. There was no variation in the serum TNF-alpha level when the same serum from a patient was assayed on different occasions. The storage of sera samples at - 700C for a period of 12 months did not result in the variation of TNF-alpha levels in any patient. Discussion Several modes of the therapeutic action of IVIg have been described in patients with demyelinating diseases. These include: (a) down regulation of cytokine production;[8] (b) IVIg induces a dose-dependent decrease in the level of TNF-alpha, interleukin - 1b (IL-1b);[9] (c) blockade of the Fc receptors of the macrophages could inhibit the macrophage-mediated phagocytosis of the antigen-bearing target cells such as myelin and this process could promote macrophage-mediated demyelination;[10] blockade of the Fc receptor on the phagocytic cells, induced by the infused IVIg could also inhibit the antibody-dependent cell-mediated cytotoxicity-a process that may render the sensitized phagocytic cells unable to exert their action;[11] (d) IVIg inhibits the complement- mediated immune damage to the capillaries;[12] (e) IVIg can suppress the antibody-dependent cytotoxicity;[13] (f) IVIg decreases the natural killer function.[14] (g) IVIg inhibits autoantibody production;[15] (h) IVIg neutralizes pathogenic antibodies.[16] Despite the above mentioned mechanisms, the precise immunomodulatory mechanism of the action of IVIg have not been well understood. This study demonstrated that elevated levels of serum TNF-alpha occur in a proportion of patients with GBS. The two studies published earlier have also emphasized the elevated levels of serum TNF-alpha in patients with GBS.[3],[4] Both these studies highlighted that the elevated levels of serum TNF-alpha correlated with the disease severity and that the elevated levels of TNF-alpha return to normal parallel with the clinical recovery. Whether TNF-alpha is directly involved in the pathogenesis of GBS or it is a result of other basic processes still remains unclear. Apart from the myelinotoxic effect, TNF-alpha in GBS could play an important role in modulating vascular endothelial function, an effect that would contribute to the development of nerve lesions in GBS. TNF-alpha can also induce endothelial cell damage.[17] Alteration in the endothelial homeostasis increases vascular permeability and this will result in the breakdown of the blood-brain barrier. All these mechanisms play an important role in the pathogenesis of GBS. The data of this study suggest that the elevated levels of serum TNFa in patients with GBS decreased following a complete course of IVIg therapy. There was a positive correlation between neurological recoveries and a decrease in the serum TNF-alpha concentration in all the 22 patients with GBS. In-vitro studies have conclusively showed a decrease in TNF-alpha concentration when sera from patients with GBS were incubated with IVIg. In this study, we observed a positive correlation in the results of the in-vivo and in-vitro studies. The relatively high TNF-alpha values in in-vivo studies may be due to the activation of T- lymphocytes and monocytes as well as concurrent TNF-alpha production during the course of the disease. The results of the in-vitro study also indicated that IVIg neutralized the TNF-alpha concentration. The in-vitro study was precisely designed to assess the reproducibility of the results as observed in the in-vivo study. In conclusion, the results of this study also indicate that IVIg therapy is particularly indicated in those GBS patients with elevated serum TNF-alpha levels. The serum TNF-alpha monitoring during IVIg therapy can also be used as one of the markers of neurological recovery in GBS patients. Although plasma exchange (PE) is another therapeutic modality, we consider that IVIg therapy is less cumbersome than PE and hence we recommend the use of IVIg in the management of GBS. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=487;epage=489;aulast=Reuben The following images related to this document are available:Photo images[ni03157t1.jpg] |
| |||||||||

{kind=link}