 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
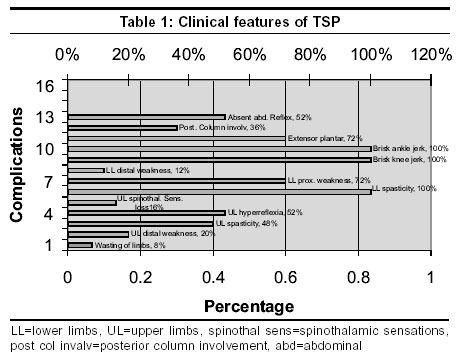
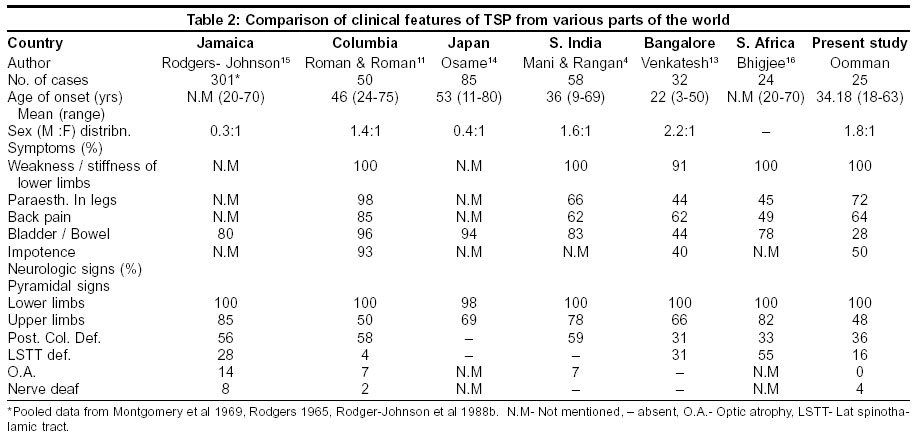
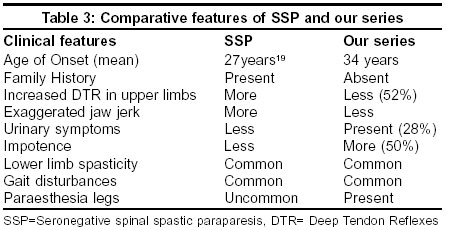
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 493-496 Original Article Tropical spastic paraparesis in Kerala, South India Oomman A, Madhusoodanan M Professor of Neurology, Medical College Kottayam Code Number: ni03159 Abstract Tropical Spastic Paraparesis (TSP) is an uncommon myeloneuropathy with an insular geographic distribution. In 1985, Human T-lymphotropic virus type I (HTLV-1) was reported to be a possible etiological factor.1 We did an epidemiological, clinical and virological study of 25 cases of TSP. They were predominantly young adult men, whose duration of illness ranged from 6 months to 15 years. Difficulty in walking, stiffness of legs and paraesthesia of legs were the main symptoms. None had tuberculosis, syphilis, malnutrition or lathyrism. Pyramidal signs of the lower limbs, upper limbs, posterior column involvement and spinothalamic tract dysfunction were the common signs. Laboratory findings and cerebrospinal fluid analysis were normal in most. Myelograms or MRI were normal in all. Only 1 case repeatedly tested positive for HTLV-1 antibodies. None of his relatives had clinical or virological evidence of TSP or HTLV-1 infection. Based on our study, we could not link HTLV-I infection to TSP in Indian cases. Virological testing for HTLV-I infection by polymerase chain reaction may be a better tool to reveal such an association. Our cases were similar to seronegative spinal spastic paralegia. A related new retrovirus or an altered immune response to HTLV-1 due to environmental or dietary factors are possibilities which require further exploration.Introduction Tropical Spastic Paraparesis (TSP), a myeloneuropathy, was reported in the last few decades. The etiological factors implicated are lathyrism, chronic cyanide intoxication due to consumption of cassava, malnutrition, and infections. The association between human T-lymphotropic virus type I (HTLV-1) and TSP opened new vistas in its etiology and epidemology. The first Indian report of TSP was published in 1969.[2] The epidemiological, clinical and pathological features of cases from India are similar to the descriptions from the rest of the world. Attempts to link TSP and HTLV-1 have not been successful[3],[4],[5],[6],[7] although the presence of HTLV-1 infection has been reported in Indian cases.[8],[9] TSP has not been reported from Kerala, the southern state of India, to the best of our knowledge. We report the results of an epidemiological, clinical and virological study of TSP in Kerala. Material and Methods This study was carried out on 25 patients in the Department of Neurology, Medical College, Kottayam, Kerala, south India. Patients with non-compressive myelopathy proven by a myelogram, computerized tomography (CT) and magnetic resonance imaging (MRI) were assessed for TSP. The criteria by Arango et al[10] were followed for diagnosing TSP. The relatives of patients with HTLV-1 antibodies were separately evaluated. A detailed history including the onset, duration and evolution of the disease was taken. Family history of neurological illness, history of extramarital sexual exposure, abortion and blood transfusions was taken. Dietary history was taken in detail, with emphasis on strict vegetarianism, lathyrus and cassava consumption. Socio-economic status, housing and sanitary conditions and consanguinity were also noted. A detailed general examination and a meticulous neurological assessment were done. The following investigations were done in all patients: hemoglobin concentration, total and differential leucocyte count, erythrocyte sedimentation rate (ESR), peripheral smear, fasting and postprandial blood sugar, renal and liver function tests, and serological test for syphilis. Cerebrospinal fluid studies were done in all patients. Cell count, protein, glucose, bacterial culture and serological test for syphilis were carried out. All patients underwent conventional myelography. Two each had CT and MRI scans. The serum samples of all the patients and controls were tested for HTLV-1 antibodies by the serodia technique. Patients admitted to the neurology ward with disorders other than non-compressive myelopathies were taken as controls. Twenty-five of them were assessed clinically, radiologically and virologically. Results A total of 25 patients with TSP were identified. At presentation the age of the 25 patients ranged between 18 and 73 years. The peak incidence was in the age group of 25 - 35 years. There were 16 males and 9 females (M:F = 2:1). Twenty-two patients (88%) were from a rural background. Symptoms and Signs The general examination was non-contributory. Neurological deficits seen in the 25 patients are summarized in [Table - 1]. Investigations CSF examination showed a normal count in 23 out of 25. CSF glucose was normal in all. The total count was less than 10/mm3 and the protein less than 75 mg% in the 2 cases with abnormal results. Myelograms and spinal X-rays were normal in all. Spinal CT and MRI were done in 2 patients each and were normal. Only 1 patient tested repeatedly positive for HTLV-1 antibodies by the serodia method in both blood and CSF. The relatives of the positive patient were evaluated and all were negative for HTLV-1 antibodies. All the controls were negative for HTLV-1 antibodies. Discussion TSP has been reported from different parts of the world including Jamaica, Martinique, Seychelles, Colombia and Japan and the clinical features appear to be uniform in these reports.[11] TSP predominates in 2 races, Japanese and Black Africans, although Caucasians, Hindus and Orientals are also affected. Blacks share a common origin from with the slave societies imported from Africa. HTLV-1 might have been brought to Japan by Portuguese traders who came along with African slaves and monkeys.[12] It is interesting that Kerala had regular trade contact with Africa and Europe for the past many centuries. A few studies from different parts of world and India[4],[11],[13],[14],[15],[16] are compared in [Table - 2]. The mean age of onset was 34 years in our study which is lower than the worldwide pooled data of 42 years.[17] The incidence of urinary disturbance and impotence in males was much lower in our study than that reported from Jamaica,[17] Colombia[11] and Japan.[14] In our study, none had retrobulbar neuritis, cerebellar signs or peripheral neuropathy. The association of HTLV-1 and TSP was first reported by Gessain et al in 1985 in 60% of cases that were seropositive. A more recent Brazilian study showed only 36% seropositivity.[18] The absence of HTLV-1 antibodies in TSP patients led to the term “seronegative spinal spastic paraparesis” (SSP)[19] being coined. Comparison of HTLV-1-associated myelopathy and SSP showed that SSP patients were young (mean age of onset: 27 years) males.[19] Positive family history, increased jaw jerk and deep tendon reflexes in the upper limbs were more common in SSP. Our patients had many features similar to SSP. The comparative features of SSP and the cases in our series are given in [Table - 3]. HTLV-1 infection is associated with a variety of human diseases including adult T-cell leukemia (ATL) and non-neoplastic inflammatory diseases. The latter includes HTLV-1 associated myelopathy / tropical spastic paraparesis (HAM/TSP) and HTLV-1 uveitis (HU) and other diseases with unestablished associations such as arthropathy, pneumopathy, dermatitis and myositis.[20] Seroprevalence of HTLV-1 in relatives of patients of HAM/SP is 29%.[21] It has been suggested that saliva cells, lymphocytes and epithelial cells may potentially participate in the oral transmission of HTLV-1.[22] TSP has been reported in India earlier.[2],[4] Kerala, a state in south India, had early contacts with Portuguese traders. However, TSP has never been reported from Kerala, unlike Japan where HTLV has been postulated to be brought by Portuguese traders. Many studies could not prove the association of HTLV-1 with TSP in India.[3],[4],[5],[6],[7],[13] The mere absence of HTLV-1 antibodies proven by serological methods cannot exclude HTLV-1 infection. There are reports of the detection of HTLV-1 by PCR after being considered seronegative for HTLV-1 on the basis of ELISA and Western blot evaluation.[23] Sequence alignments and comparisons indicated that the HTLV-1 strains from southern India were 99.2% to 100% identical among themselves and 98.7 to 100% identical to the Japanese prototype HTLV-1 ATL.[24] A high prevalence (40%) of HTLV-1 antibodies in wild-caught bonnet monkeys in south India has been reported.[10] Conclusions Tropical spastic paraparesis (TSP), a chronic non-compressive myelopathy is present in Kerala, south India. Clinical features are generally similar all over the world with mild differences. HTLV-1 could not be definitely linked etiologically to cases of TSP in our series. HTLV-1 has not been linked to cases of TSP reported from the rest of India. Our cases had many similarities to seronegative SSP. The high prevalence of HTLV-1 in south Indian wild-caught monkeys raises the possibility that HTLV-1 may be endemic in this region. The paucity of HTLV-1 antibody positivity is a striking feature in our series. PCR may identify HTLV-I in seronegative cases. In the absence of PCR, our conclusions are not definite and it constitutes a drawback of this study. The clinical and serology profile raises interesting possibilities of a similar retroviral infection or environmental or dietary factors modifying the immunological response to HTLV-1 to cause the observations in our series. Further research is needed in these areas.References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=493;epage=496;aulast=Oomman The following images related to this document are available:Photo images[ni03159t2.jpg] [ni03159t1.jpg] [ni03159t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}