 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
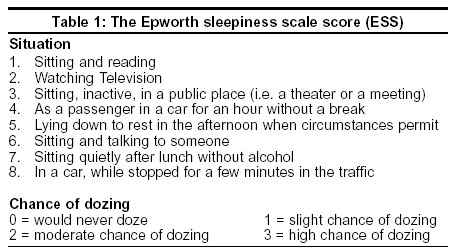
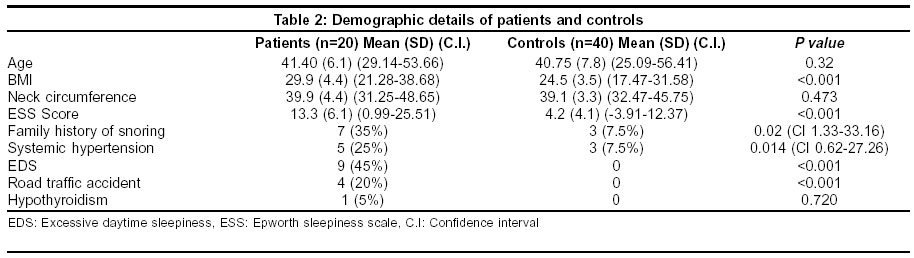
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 497-499 Original Article Obstructive sleep apnoea: A case-control study Pradeep Kumar VG, Bhatia M, Tripathi M, Srivastava AK, Jain S Department of Neurology, All India Institute of Medical Sciences, New Delhi - 110029 Code Number: ni03160 Abstract Introduction: Obstructive sleep apnoea (OSA), is characterized by loud snoring and excessive daytime sleepiness. Though the gold standard for diagnosis is overnight polysomnography (PSG), sleep questionnaires have also been used to diagnose this with good predictive value. Material and Methods: A pre-designed proforma with clinical details, symptom-specific questions for diagnosis of OSA, and Epworth Sleepiness Scale (ESS) was administered to 20 patients presenting to the Sleep Disorder Clinic of our hospital and to 40 age and sex-matched relatives (control group). The students ‘t-test’ and chi-square were used as the statistical tests. Results: There were 20 patients with a mean age of 41± 8 years, and 40 controls with a mean age of 41 ± 6 years (P=>0.05). Seven had family history of snoring in the study group and 3 in the control group (P=0.02). Four had met with road traffic accidents in the study group and none in the control group (P=0.001). The body mass index (BMI) was 29.9 (SD 4.4) in the study group and 24.5 (SD3.5) in the controls (P=0.001). The mean ESS was 13.3 ± 6 in the patients and 4.2+ 4 in the controls (P=0.001). A larger number of patients with OSA had hypertension: 5/20 vs. 3/40 (P=0.01). Conclusion: Patients with OSA had significantly higher BMI and ESS score, and were more likely to have hypertension and road traffic accidents. Increased awareness of this entity is essential.Introduction Obstructive sleep apnoea (OSA) is a condition characterized by repeated episodes of upper airway closure during sleep. It is associated with a constellation of symptoms and objective findings which include loud snoring, motor restlessness, unrefreshing sleep and excessive daytime sleepiness (EDS).[1] The prevalence of this condition is about 2% and 4% in women and men respectively.[2] OSA is associated with significant morbidity and mortality, both from vascular complications and from road traffic and industrial accidents.[3] The Epworth sleepiness scale (ESS) score is a simple tool to determine the degree of EDS in patients with OSA.[4] The diagnostic test for OSA is an overnight polysomnography (PSG).[5] Respiratory distress index (RDI), which is the average number of respiratory disturbances per hour of sleep, of more than 5 is considered to be diagnostic of OSA.[2],[6] However, these diagnostic tools are costly, time-consuming and of limited availability, particularly in developing countries. OSA has been diagnosed in previous studies using a sleep questionnaire designed to assess the specific symptoms associated with sleep-related breathing disorders with higher predictive ability, with additional data on body mass index (BMI).[7] This is of special relevance to our country where the initial diagnosis of OSA can be made using a questionnaire and then the patients can be subjected to PSG for confirmation and assessment of severity. In the present study, we used a questionnaire to identify patients with OSA, evaluated their clinical profile and administered ESS for evaluation of EDS. Material and Methods Fifty-eight patients were evaluated in the Sleep Disorders Clinic, All India Institute of Medical Sciences, New Delhi, between January and December 2000. Out of these, 20 patients were clinically diagnosed to have OSA and they formed the study group. The control group was formed by 40 age and sex-matched subjects who were relatives of patients attending the Neurology outpatient department. A detailed clinical history was taken in a pre-designed proforma which included family history of snoring up to three generations, a sleep questionnaire for symptoms of OSA,[8] which was modified from the Cleveland Veterans Affairs Hospital sleep questionnaire, and the ESS score questionnaire [Table - 1]. The sleep questionnaire contained symptom-specific questions for various sleep disorders including OSA. It contained 30 questions of which 6 were for the diagnosis of OSA. They were: presence of snoring, long pauses in breathing during night, motor restlessness, excessive daytime sleepiness, feeling unrefreshed after night sleep and presence of morning headache. The questions carried definite scores (0-4), score (1) rarely, score (2) 1-2/week, (3) 3-4/week and (4) always, based on the frequency of the occurrence of symptoms and 0, if the patient was asymptomatic. Patients with score 3 or more on the questions were diagnosed to have OSA. The questions for associated medical illnesses included those for systemic hypertension, hypothyroidism, coronary artery disease and chronic obstructive airway disease. The ESS was administered to all the patients and controls. The ESS questionnaire is a simple tool to assess the general level of daytime sleepiness (average sleep propensity). ESS measures the probability of falling asleep in eight situations (Scores 0-3; total score of 24). Complete physical examination was done in all the patients and controls with specific reference to the BMI, neck circumference, ear, nose, throat examination and blood pressure recording. Routine investigations such as complete hemogram, serum biochemistry, thyroid function tests (TFT), chest X-ray, and ECG were done in all the patients. Statistical Analysis Results All the patients were men, with a mean age of 41 ± 8 years and duration of symptoms of 6 ± 2 years. All had history of snoring, with EDS. There was history of witnessed apnoea in 9 patients, feeling unrefreshed in the morning in 14 patients and headache on awakening in 8 patients. Positive family history of snoring was present in 7 (35%) patients, history of road traffic accident in 4 (20%) and hypothyroidism in 1 patient. Systemic hypertension was present in 5 (25%). ECG showed evidence of left ventricular hypertrophy in 5 (25%) and chest X-ray was normal in all the patients. The mean BMI was 29.94 ± 4.37 and the neck circumference 39.9 ± 3.3 in the study group. The mean ESS score was 13.3 ± 6.1 in the study group. The mean age of the control group was 40.8 ± 6.1. There was positive family history of snoring in 3 (7.5%). None had history of road traffic accidents and 3 (7.5%) had systemic hypertension. The mean BMI of the control group was 24.32 ± 3.53, neck circumference was 39.1 ± 4.4 and the ESS score was 4.2 ± 4.1 [Table - 2]. Discussion OSA is a common sleep disorder characterized by recurrent episodes of apnoea during sleep associated with snoring, motor restlessness, and EDS.[1] In spite of the advances in diagnostic facilities, the published data on OSA from India are limited.[9] This is the first study from India comparing risk factors in patients with OSA and controls. The risk of OSA increases with age and is strongly correlated with obesity and male gender.[10],[11],[12],[13] Its prevalence reaches a maximum between the fifth and sixth decades.[14] The mean age of patients in the present series was 41± 6 years and all were men. Family history of snoring was present in 35% of the cases in our series and it was significantly higher than in the controls. Familial aggregates of OSA indicate that risk factors for the development of this condition may exist very early in life.[15],[16],[17] Untreated OSA is associated with a prevalence of chronic hypertension in excess of 40%, whereas approximately 30% of all idiopathic hypertensives have OSA.[6] A significant increase in the systemic arterial pressure occurs cyclically with episodes of apnoea, with maximum elevation occurring after the resumption of ventilation.[18] In our study 25% had systemic hypertension which was significantly higher when compared to the control group (7.5%). OSA is associated with an increase in BMI, which is a measure of obesity. Obesity degrades waking and sleeping ventilation, in addition to the upper airway dynamics.[19] Adiposity compromises the upper airway by altering and reducing the airspace by infiltration of parapharyngeal structures.[20] Also, adipose tissue deposition around the abdomen, diaphragm and ribs reduces thoracic cage compliance, leading to increased effort to breathe. Functional residual capacity is decreased and atelectasis of the dependent airway creates ventilation and perfusion mismatch with hypoxemia. This is aggravated in the supine position, when abdominal weight creates an additional load.[19] In the present series, the BMI of the patients was 29.9 ± 4.4 which is significantly higher than controls 24.5 ± 3.5. BMI more than 25 kg/m² was observed in 16 of the 20 patients in this study. There was no statistically significant difference in the neck circumference between the study group and the control group. Road traffic accidents, secondary to EDS, are a cause of significant morbidity and mortality at the workplace and on the roads.[21],[22],[23],[24] A history of road traffic accidents was obtained in 4 patients (20%) with OSA. Previous reports have documented the risk to be 7 times that of the general population.[24] Nine patients complained of EDS, which was significantly higher than the controls. The ESS score was significantly higher in the study group as compared to the controls. EDS is the cardinal daytime symptom of OSA, which manifests as a tendency to inadvertently fall asleep during quiet or passive activities, to take intentional naps, or to experience short but repetitive alternative lapses while doing monotonous tasks. Such sleepiness is the consequence of sleep fragmentation secondary to sleep apnoea during the night. In one of the largest series of sleep apnoea syndrome, EDS was reported in 83% patients.[25] The ESS score was significantly higher in our study group as compared to the controls. ESS has been used as a measure of severity of EDS in previous studies; it correlates with the severity of OSA.[26] This study is questionnaire-based and hence has the limitation of underdiagnosing patients with mild OSA. However, moderate and severe OSA can be efficiently diagnosed by the sleep questionnaire.[8] The present study also underscores the relationship of OSA with systemic hypertension, increased BMI and road traffic accidents, thus stressing the need for its diagnosis and appropriate management. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=497;epage=499;aulast=Pradeep Kumar The following images related to this document are available:Photo images[ni03160t2.jpg] [ni03160t1.jpg] |
| |||||||||

{kind=link}
{kind=link}