 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
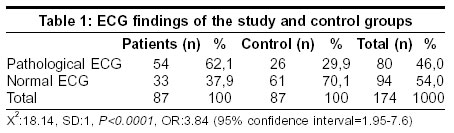
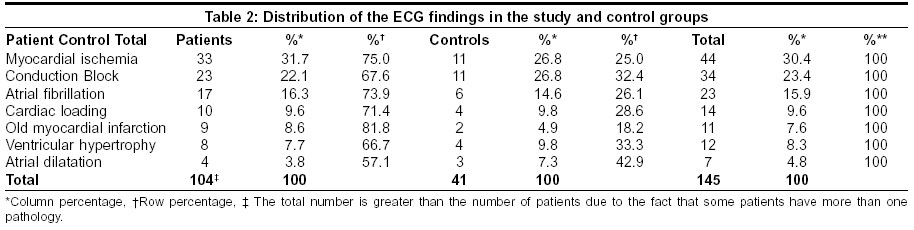
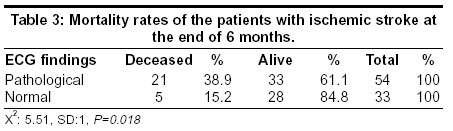
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 500-502 Original Article Electrocardiographic findings and prognosis in ischemic stroke Bozluolcay M, Ince B, Celik Y, Harmancí H, Ilerigelen B, Pelin Z Istanbul University, Cerrahpasa Medical School; Department of Neurology, Istanbul Code Number: ni03161 Abstract Introduction: Electrocardiographic (ECG) changes are observed in patients with acute stroke and are related with the prognosis. Aims: To determine the frequency and significance of ECG changes in patients with acute ischemic stroke. Material and Methods: In a prospective hospital-based study 87 patients with cerebral infarction were observed for ECG changes during their stay in the hospital. All the patients had ischemic stroke for the first time. The ECG changes observed were compared with those of the control group consisting of 87 patients. Results: Of the 87 patients of the study group, 47.1% were females and 52.9% males. The mean age was 65.5 ± 11.9 (range 31–91 yrs). The control group consisted of 50.6% females and 49.4% males. The mean age was 64.5 ± 11.9 (range 31–87 yrs). The frequency of the ECG changes observed in patients with cerebral infarct was 62.1% while it was 29.9% in the control group (P<0.0001). ECG changes observed were mostly related to myocardial ischemia. The six-month mortality rate in the patients with ECG changes was 38.9% whereas it was 15.2% in those with normal ECG (P<0.05). Conclusions: The observations of this study suggest that cardiac evaluation in patients with acute ischemic stroke is of prognostic importance.Introduction The effect of brain injury on the heart was demonstrated in experimental animals in the 1930s.[1] Cardiac changes in patients with acute stroke were first reported in 4 patients in 1947.[2] Subsequently, several studies investigated the effect of brain injury on the heart and very few studies addressed the issue of the prognostic significance of these changes.[2],[3] On the other hand, the relation between the heart and cerebrovascular diseases has been well studied.[4],[5],[6],[7],[8],[9],[10] In this study, ECG changes and their prognostic significance was studied in patients with acute ischemic stroke.Material and Methods Eighty-seven consecutive patients with first ever-acute ischemic stroke admitted to the neurology wards of the Medical School, Cerrahpasa, between October 1995 and June 1996 were included in the study. The control group included 87 patients admitted to other wards for some ailment other than cerebrovascular diseases and patients were matched by age. Patients admitted to cardiology wards were excluded from the control group. Hemorrhagic strokes, brainstem ischemic strokes, and strokes related to trauma were excluded from the study. Diagnosis of cerebral infarction was established in all the patients by cranial tomography (CT) and/or magnetic resonance imaging (MRI). Detailed history and neurologic findings were recorded in all the patients. All the patients were evaluated for cardiac disease by detailed history and clinical examination. ECG findings done on the day of admission were considered for the analysis. Consultant cardiologists analyzed the findings. ECG abnormalities were grouped into myocardial ischemia, old myocardial infarction, atrial fibrillation, ventricular hypertrophy, atrial dilatation, cardiac loading, and conduction block. Follow-up data regarding death was collected from the relatives of the patients either by personal interview in the clinic or by telephonic interview. Mortality figures within 30 days of the onset of stroke and also at six months were collected. The statistical significance was determined using the chi-square test. Results The study group consisted of 41 (47.1%) females and 46 (52.9%) males and the mean age of the patients was 65.5 + 11.9 years (range 31-91). The control group had 44 (50.6%) females and 43 (49.4%) males and the mean age was 64.5 + 9.1 years (range 31-87). The frequency of ECG abnormalities was 62.1% in the study group and 29.9% in the controls (P<0.0001) [Table - 1]. In the study group ECG changes suggestive of myocardial infarction (37.9%) were the common findings followed by atrial fibrillation (19.5%). Whereas in the control group the corresponding figures were 12.6% and 6.8% respectively [Table - 2]. Clinical evaluation revealed underlying cardiac disease in 41.3% of the study group and 14.9% of the control group. Thirty-day mortality was 14.8% in the patients with ECG abnormalities whereas it was 8.5% in the patients without ECG abnormalities (P<0.05). The overall mortality rate at the end of this interval was 29.8%. Mortality at six months of follow-up was significantly higher in patients with ECG changes when compared to those patients without ECG changes (P<0.05) [Table - 3]. Discussion Coronary heart disease and ischemic stroke share the same risk factors and may coexist in the same patient and in most of the patients with ischemic stroke, the mortality may be related to the underlying coronary heart disease.[1] ECG changes are common in patients with ischemic stroke. In this study patients with brainstem ischemic stroke were excluded for the reason that lesions involving the medulla oblongata may be associated with autonomic dysregulation and hemodynamic instability.[11] ECG features suggestive of myocardial ischemia were the common findings seen in this study. The findings in other studies were similar.[12],[13] The reported frequency of new ECG changes in patients with acute ischemic stroke was 15-30%.[1] In our study 41.3% of the patients were clinically diagnosed as having a cardiac disease and in the remaining the diagnosis was based on the ECG findings. Given the fact that these patients had no earlier history or laboratory evidence of cardiac disease, it was very difficult to determine what proportion of the ECG changes were related to acute cerebral infarction. However, the fact that ECG abnormalities observed were significantly higher in the study group when compared to the control group suggests that some of the changes observed in the study group might be related to acute cerebral infarction. Autopsy studies of the heart in patients who died following acute stroke showed widespread myocardial necrosis and hemorrhagic lesions, referred to as “myositolisis”. These lesions were detected near the nerve endings suggesting possibly neurogenic in origin.[1],[14] In a patient with ECG findings suggestive of acute myocardial ischemia, who died due to recurrent cerebral bleed, autopsy study showed no coronary arterial pathology.[15] In another study there was no evidence of coronary artery disease at autopsy in 8 patients with ECG changes following acute stroke.[2] Studies have shown that the frontal lobe, insular cortex and amygdala play an important role in the regulation of the heart via the (sympathetic and parasympathetic systems and cardiac involvement is more common in patients with cerebral lesions involving these areas.[3],[8],[16],[17],[18],[19] The possible pathogenesis of cardiac arrhythmias in patients with acute ischemic stroke is autonomic system activation.[1],[13] However, in this study we have not correlated the ECG changes with the anatomical location of CT infarct. Cardiac arrhythmias are the most frequently found ECG abnormalities in patients with stroke.[8] In the study by Natelson[20] cardiac arrhythmias were noted in 61% of patients with all types of strokes, in 78% of hemorrhagic strokes, and 51% of ischemic strokes, whereas they were observed in only 15% of the control group.[20] The reported frequency of new onset cardiac arrhythmias in patients, both with ischemic and hemorrhagic stroke without underlying cardiac disease is 25-40%.[2] The detection of arrhythmias can be higher if the patients are followed with a Holter.[2] Findings of ventricular hypertrophy and other evidence of volume load in the ECG probably reflect the preexisting cardiac disease rather than the consequence of acute cerebral infarction. The most common cause of death in patients with stroke is cardiac.[1] In our study both 30-day mortality and mortality at 6 months was significantly high in patients with ECG changes. Earlier studies suggest that new ECG changes in the acute phase of stroke are associated with higher mortality.[2] The effects of acute cerebral infarction on the heart are temporary.[1],[6] In our study none of the patients with ECG evidence of cardiac arrhythmia and myocardial ischemia received any specific treatment. Patients with preexisting heart disease had appropriate treatment. To determine the effect of new onset ECG changes in patients with acute cerebral infarction on the immediate and long-term mortality, well-designed randomized control studies are essential. This study suggests that cardiac status and also ECG changes in patients with acute ischemic stroke are associated with higher mortality. We also feel that long-term cardiac monitoring is mandatory in patients with acute stroke, particularly in patients with cardiac and ECG abnormalities till the ECG changes stabilize or resolve. Such studies are likely to throw light on the possible pathogenesis of the acute onset ECG changes and also their effect on mortality. This also may provide opportunities for appropriate drug management. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=500;epage=502;aulast=Bozluolcay The following images related to this document are available:Photo images[ni03161t1.jpg] [ni03161t3.jpg] [ni03161t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}