 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
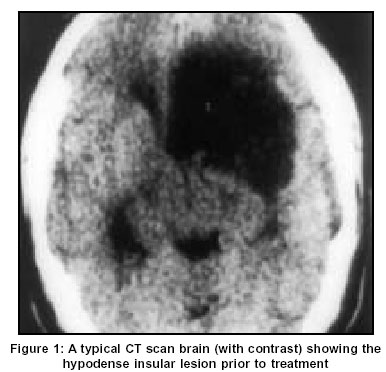
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 503-506 Original Article Radiological and clinical outcome following stereotactic biopsy and radiotherapy for low-grade insular astrocytomas Shankar A, Rajshekhar V Department of Neurological Sciences, Christian Medical College and Hospital, Vellore - 632004 Code Number: ni03162 Abstract Thirty patients with low-grade (WHO Grade II) astrocytomas involving the insula, who had undergone stereotactic biopsy followed by radiotherapy, were followed up to evaluate the outcome with regard to control of seizures, memory and language function, Karnofsky Performance scale and regression in tumor volume. Patients were followed up for a mean of 27.8 months, during which time they showed improvement in all the factors that were studied. A statistically significant change was, however, seen only in the reduction in tumor size, probably due to the small sample size and the short duration of follow-up. Stereotactic biopsy followed by radiation therapy provides a good short-term outcome in patients with low-grade insular astrocytomas.Introduction The insular lobe or the Island of Reil was first referred to by Vic d'Azyr in 1786 as the “convolutions situated between the Sylvian fissure and the corpus striatum”.[1] The first description was done by J. C. Reil in 1809 and further detailed anatomic descriptions of this structure were made independently by Guldberg and Eberstaller in 1887.[2] Gliomas involving the insula have traditionally been conservatively managed, with only biopsies being done, followed by radiotherapy, for fear of injuring the middle cerebral artery or its branches.[3],[4] The possibility of damage to the highly eloquent cortex (on the left side) and the close proximity of the internal capsule and basal ganglia, with the danger of accidental damage to these structures, are the other reasons for this approach. We planned to study the clinical and functional outcome following stereotactic biopsy and radiation therapy for patients with low-grade insular astrocytomas. Material and Methods Patients with histologically proven low-grade (WHO Grade II[5]) astrocytomas primarily involving the insula, who had undergone stereotactic biopsy and radiotherapy between January 1993 and March 2000 were included in the study. The study consisted of a retrospective (till November 1997) and a prospective component. Patients belonging to the retrospective group, in whom no follow-up was available, were excluded from the study. Patients who could be included in the prospective group were identified on admission to the hospital and underwent a detailed evaluation before the procedure. If the biopsy was confirmatory, they were evaluated both clinically and radiologically at each review visit. All patients underwent a full neurological examination with detailed seizure history. Evaluation of memory was done using the Post Graduate Institute (PGI) scale and of language by the expressive speech, receptive speech, reading and writing scales of the Luria-Nebraska Neuropsychological Battery (LNNB). Both these were translated into the patients' language so as to reduce errors. Assessment of the Karnofsky Performance Scale (KPS)[6] was done either during clinical examination, or based on patients' responses to the questionnaire. The volume of the tumor was calculated from the CT scans [Figure - 1] using the Cavalieri direct estimation method.[7] Patients in the retrospective group were identified by analysis of hospital records and CT scan images. Follow-up was obtained in one of three ways:
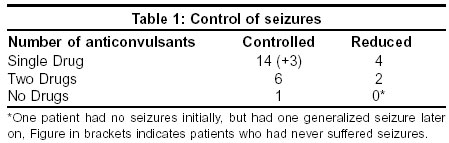
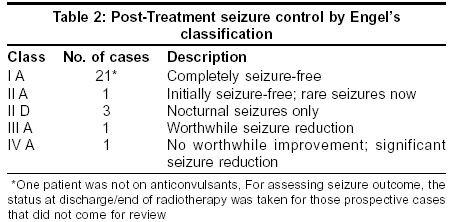
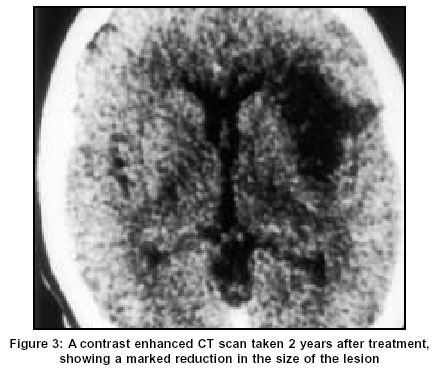
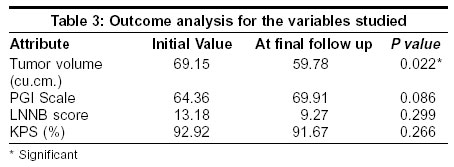
There were 16 patients in the prospective group and 22 patients in the retrospective group. Eight cases were excluded from the retrospective study due to lack of follow-up data, leaving a total of 30 cases. Prospective cases who did not come for long-term follow-up were included in the study as data regarding seizures and KPS were available till the date of completion of radiotherapy. There were 11 males and 3 females in the retrospective group while the ratio was 10:6 in the prospective group. Nine patients in each group had a left-sided lesion. The largest number of patients (12) belonged to the 31-40 years age group, with 8 patients each in the 21-30 and 41-50 years groups. The mean duration of follow-up in the study was 27.8 (+/-20.86) months. The prospective patients were followed up for a mean of 20.4 months (+/- 5.54 months) and the retrospective cases for 33.64 months (+/- 26.38 months). Results Follow-up was possible to a variable degree in each of the 30 patients. While the seizure outcome could be calculated for 27 (3 patients were seizure-free), the KPS could be evaluated for 25 cases. Follow-up CT scans were available for 17 cases. The LNNB and PGI scales could be evaluated on follow-up for only 11 patients. Of these 11, 2 were retrospective cases that were evaluated more than once. For these 2 cases, the first set of data obtained on follow-up was considered to be the initial data for analyzing memory and language functions. Seizures were the presenting symptom in 11 out of 14 retrospective cases and in 15 out of 16 prospective cases. One of the patients in the retrospective group who had initially been seizure-free suffered one attack of generalized seizures 4 years after the biopsy. Out of these 27 cases, 15 patients had generalized tonic-clonic seizures, 6 had complex partial seizures and 6 had focal motor seizures. Of these, 18 patients were on a single anti-convulsant drug, with control of seizures in 14. The 3 patients who had not had seizures were also on monotherapy. There were 8 patients on two drugs, given in various combinations. The drugs used were phenobarbitone, carbamazepine, phenytoin and sodium valproate [Table - 1]. On subdividing these patients using Engel's seizure outcome classification,[8] all but 2 cases were found to have a favorable outcome [Table - 2]. Eighteen patients had CT scans done during follow-up. A reduction in tumor size was seen in all but one patient [Figure - 2]& [Figure - 3] . None of the patients in this study had contrast enhancement in the initial CT scan. Two patients developed contrast enhancement 3 years and 7 years following the initial treatment, and 1 of them was symptomatic. Both patients were started on chemotherapy with CCNU. The second patient was doing well one year later while the former did not come for a further review. Complete memory and language function testing was carried out in 11 patients. Six patients showed a slight improvement in LNNB while the score worsened in 3 and remained the same in 2 patients. On the other hand, 7 patients showed an improvement in the PGI scale, while 4 deteriorated. The KPS improved marginally in 1 and worsened in 3 patients, while it remained the same in all the others. Statistical analysis of the results was done using the t-test for paired samples. A significant difference was noted between the volumes of tumor on the initial and follow-up CT scans (P=0.022). While some trend towards the improvement of memory and language function was noted during follow-up, these changes were not statistically significant. No such difference was noted in the KPS [Table - 3]. Discussion Despite the complexity of its anatomical relationships and functions, surprisingly little is known about the sequelae of damage to the insular lobe.[9] The most persistent finding associated with damage to the insula has been complex partial seizures, especially with involvement of the visceral sensations.[2] Cases of insular damage with variable involvement of the superior temporal gyrus and inferior parietal region have presented with conduction aphasias. Infarction of the anterior insula may result in difficulty in initiation of speech. Patients with infarction of the insula have revealed global aphasia when the dominant lobe was involved. Involvement of the non-dominant lobe resulted in mutism, neglect, apraxias or bilateral opercular syndromes. Other deficits include object naming and articulatory planning deficits, auditory processing disorders, ictus emeticus and dyslexia.[10],[11],[12],[13],[14],[15] Insular gliomas may be confined to either the anterior or posterior parts or may involve the entire insula, without infiltration of the adjacent opercular gyri or the basal ganglia. This propensity to spread within the confines of the allocortex and mesocortex, sparing the adjacent neocortex and medullary structures, suggests an affinity of these tumors for phylogenetically primitive zones (an idea introduced by Filiminoff in 1947 and developed by Yakolev in 1959). Therefore these tumors may be considered a different entity from other supratentorial low-grade gliomas.[16],[17],[18] The rationale for the use of stereotactic biopsy in cases of insular gliomas is based on the studies by Ojemann et al,[19],[20] which suggested that early in the course of the disease, most astrocytomas have a normally functioning cortex within brain tissue that appears abnormal on macroscopic examination. Their studies have shown that intrinsic brain tumors can invade cortical and subcortical structures without disrupting function. No attempt was made by us to study the survival of these patients; various studies on the effect of stereotactic biopsy followed by radiotherapy in patients with low-grade cerebral astrocytomas has reported survival rates longer than the duration of follow up in our study.[21],[22] North et al[23] reported 5 and 10-year survival rates for 55% and 43% patients with low-grade astrocytomas, respectively. Another study by Lunsford et al[24] on 35 patients showed a median survival of 9.2 years. The most extensive series on the surgical management of insular tumors was reported in 1996 by Yasargil et al,[18] who had treated 150 patients. They had noted a preponderance of left-sided tumors, as well as a high incidence of temporal lobe epilepsy as the presenting symptom. They reported a good outcome following radical surgery in 56 benign and 82 malignant tumors and a fair outcome in 4 benign and 8 malignant tumors respectively (out of a total of 60 benign and 90 malignant cases). Recurrence was documented in 8 benign and all malignant cases. Other authors have also reported favorable outcomes following radical excision of insular tumors, especially low-grade astrocytomas.[25],[26],[27] An operative morbidity of 10% and seizure control in 90% of cases was reported by Zentner et al.[28] However, preoperative angiograms to delineate the lenticulostriate artery and direct cortical stimulation to identify the internal capsule were necessary to prevent intra-operative catastrophes.[29] The use of neuro-navigation has also been reported to reduce operative morbidity.[30] An alternative mode of treatment with interstitial radiosurgery using radioiodine in the treatment of low-grade supratentorial astrocytomas has also been documented.[31] Nearly 90% of the patients in this study had at least a temporary improvement in the KPS. There have been no studies that have looked into the neuropsychological status of these patients, in order to determine whether there was any subtle deterioration or improvement following the conventional method of treatment. We decided to concentrate on the language function and memory of these patients, as many reports have shown that they may be affected in patients with insular lesions.[10],[11],[12],[13],[14],[15] The scales used were selected for their ease of administration, reproducibility and the fact that the final impression can be converted into a score, allowing easy comparison. Determining the extent to which these functions are affected can help in outlining modes of treatment, when similar studies are done on patients who undergo surgery. The KPS was added on as it could easily be ascertained by simple queries mailed to the patient. This was important as many of the patients had a poor educational status. In the short follow-up that was possible in this study, most of the patients showed an improvement in the functions studied. However, contrary to expectations, no significant difference could be demonstrated between left and right-sided lesions. The small sample size may again be the cause for this phenomenon. Conclusions Most patients with low-grade insular gliomas, undergoing stereotactic biopsy followed by radiation therapy show an improvement in all the aspects studied, namely, tumor volume, memory, language function, KPS and control of seizures, over the short term. The lack of statistical significance was probably due to the small sample size in the study. Further studies are required to predict the long-term survival and quality of life of these patients. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=503;epage=506;aulast=Shankar The following images related to this document are available:Photo images[ni03162t1.jpg] [ni03162t2.jpg] [ni03162f2.jpg] [ni03162f1.jpg] [ni03162t3.jpg] [ni03162f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
![Figure - 2]](/showimage?ni/photo/ni03162f2.jpg){kind=link}
{kind=link}
{kind=link}