 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
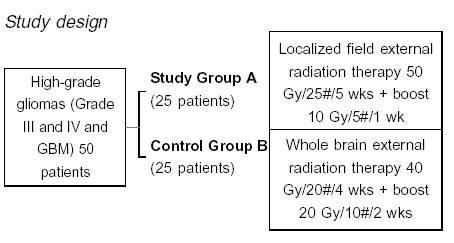
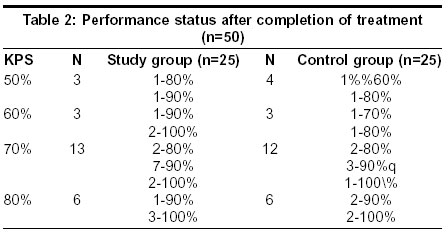
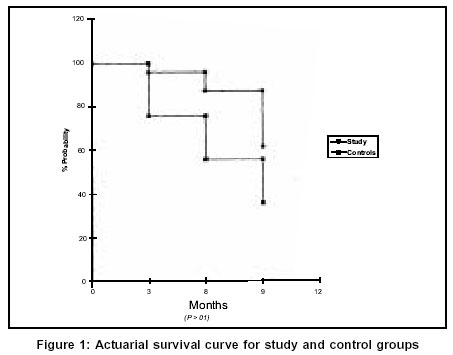
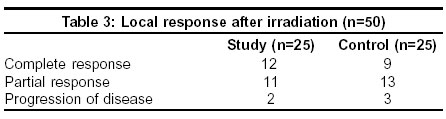
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 512-517 Original Article Local control of high-grade gliomas with limited volume irradiation versus whole brain irradiation Sharma RR, Singh DP, Pathak A, Khandelwal N, Sehgal CM, Kapoor R, Ghoshal S, Patel FD, Sharma SC Department of Radiotherapy and Oncology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160012 Code Number: ni03164 Abstract Introduction: To evaluate the role of limited field radiation therapy in the management of high-grade gliomas and glioblastoma multiforme (GBM). Material and Methods: From July ’96 to January ’98, 50 newly diagnosed patients of high-grade gliomas (Grade III and IV) and glioblastoma multiforme who underwent surgery in the form of partial, sub-total or near-total excision as the primary treatment were enrolled in this study. The patients were randomized to receive two different postoperative external radiation protocols, Study Group A: Localized field external radiotherapy 50 Gy/25#/5 wks followed by Boost 10 Gy/5#/1 wk, Control Group B: Whole brain external radiotherapy 40 Gy/20#/4 wks followed by Boost 20 Gy/10#/2 wks by localized field. Results: 20/25 (80%) patients in the study group and 14/25 (56%) patients in the control group showed improvement in their Karnofsky Performance Status (KPS). Thus a significant difference in the performance status was noted in favor of limited field irradiation. No significant difference in the local response was seen between the two groups after radiotherapy. Six months progression-free survival of the study group was 44% as compared to 26% in the control group. Six months overall survival was 66.67% in the study group and 50.72% in the control group (P<0.01). Maximum recurrences were noticed within 2 cm of the original tumor margin in both the groups. Conclusions: Although local control and survival of the patient in both the groups were same, performance status definitely improved in patients treated with localized field irradiation only. Introduction High-grade gliomas [malignant gliomas Grade III and IV, and glioblastoma multiforme (GBM)] represent 40-50% of primary intracranial tumors in adults[1] and account for approximately 20% of all pediatric neoplasms. Treatment of these patients has been a formidable challenge as the prognosis of these patients remains poor. With conventional radiation therapy, the median survival time for patients with anaplastic astrocytomas is 36 months and that for GBM is 10 months. Surgical excision is the primary modality of treatment, varying from near-total excision to a simple biopsy. Because of its proximity to the critical areas of the brain and its deeply infiltrating nature, operative resection of the tumor with generous margin of the adjacent normal tissue is often impossible.[2] External beam irradiation has a proven adjuvant role in improving the local control rates, survival,[3] and is capable of delaying the disease progression. The major causes of radiation failure are recurrence of the tumor beyond its initially delineated margins, and survival of hypoxic, non-dividing cells deep within the tumor.[3],[4],[5] The two important parameters to be considered are the volume to be irradiated and the dose to be delivered. For effective local control, doses in the range of 55-60 Gy need to be delivered. However, it is clear that with conventional fractionation i.e. 1.8-2 Gy/fraction we also approach threshold levels for central nervous system necrosis at around 60 Gy when the whole brain is irradiated.[6] Although not well documented, long-term survivors with doses of this magnitude frequently do show deficits involving short-term memory or cognitive functions. Thus it is advisable to restrict the irradiated volume to the extent possible without compromising the tumor control. A dose of 60 Gy or equivalent delivered to a precisely delineated target volume, and planning treatment volume seems to be more appropriate.[7] Only less than 1.1% of patients with high-grade glioma present with multiple lesions and so there is no potential benefit of whole brain irradiation as the standard treatment for all patients. Moreover, approximately 90% of tumors recur at the original tumor site after whole brain irradiation.[8],[9],[10],[11] With whole brain irradiation there is excessive dose to adjacent normal tissue, thereby increasing morbidity with no added advantage of better tumor control rates, thus compromising with the therapeutic ratio. Hence, limited field irradiation may offer an alternative to whole brain irradiation for GBM and high-grade glioma. There is a paucity of data relating to limited field irradiation in patients of high-grade glioma and as no randomized trials are available, a prospective randomized study was undertaken to compare the results of limited volume irradiation versus whole brain irradiation in high-grade glioma. Material and Methods Patient selection criteria
Treatment Planning and Execution For Localized Field Irradiation, target volume for treatment included gross tumor volume and a margin of 3 cm beyond the typical enhancing rim of high-grade glioma as demonstrated on the pre-operative CT/MRI. A perspex cast was made in the treatment position for immobilization of the head and simulator films were taken in the anteroposterior and lateral view and tumor volume was reproduced on simulator film with the help of CT/ MRI scan. Treatment planning was done on treatment planning system to plot isodose distribution. Appropriate field arrangements were chosen depending on the best isodose coverage of the tumor and minimal dose to normal tissue after optimization. The most common field arrangement was two lateral parallel opposing localized fields. The beam-modifying device in the form of wedge filters was used for anterolateral fields or two adjacent oblique radiation fields. A total dose of 50 Gy/25#/5 wks was planned to this treatment volume and patients were treated with megavoltage beams using a 4-6 MV linear accelerator. After the completion of 50 Gy the field was further reduced and now only a 1.5-cm margin was taken around the preoperative tumor volume. A boost of 10 Gy/5F/1 week was given to this reduced field. For Whole Brain Irradiation, a target volume in the control Group B included the whole brain to encompass the entire intracranial structures. Two lateral parallel opposing fields were used and a simulator verification film was taken and treatment planning was done on treatment planning system; the beam-modifying device was used if required as described in study Group A. A dose of 40 Gy/20#/4 wks was delivered to the whole brain on a 4-6 MV linear acceleration. After the completion of 40 Gy a boost of 20 Gy/10#/2 wks was planned with shrinkage of fields covering preoperative tumor volume with a 2-3-cm margin around the enhancing ring as seen on preoperative CT/MRI scans. Follow-up
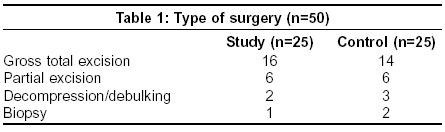
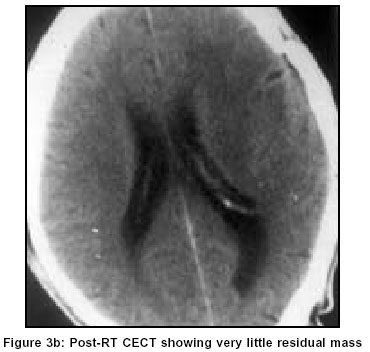
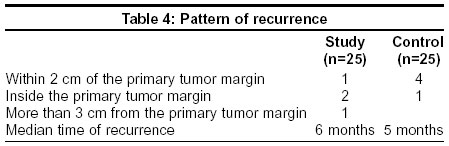
Statistical Analysis Results Type of Surgery Karnofsky Performance Status (KPS) Response Recurrence Survival Complications Discussion High-grade gliomas account for 40% of the central nervous system (CNS) malignancies and present a supreme challenge to local mode of therapy despite best advances in the field of oncology.[1] Because of their location and the diffuse nature of local spread, complete surgical excision is difficult to achieve and resection of the tumor with generous margins of adjacent normal tissue is impossible in most situations.[4] Most of these lesions infiltrate into the surrounding normal CNS tissue for a considerable distance. Hence, after surgery it is necessary to irradiate a substantial amount of normal tissue within the target volume. These tumors could be contained if sufficiently high doses could be delivered without damaging the surrounding normal brain tissue. Conventional radiotherapy of high-grade gliomas is currently under criticism regarding the dose and volume considerations. Most malignant gliomas present as solitary localized lesions and only 1.1% of patients present with multicentric lesions.[9] As high-grade gliomas infiltrate into significant distances along major white matter pathways in the majority of cases, relatively generous margins and inclusion of all the radiographic evidence of the tumors and associated edema must be the rule in designing the treatment portals for limited volumes.[12] Results of various studies show no compromise in results when limited field radiotherapy was compared to whole brain irradiation.[13],[14],[15] Similarly, the clinical trials which used volumes of about 2/3 of the brain reported survival data comparable to those reported by other study groups using whole brain irradiation.[16],[17],[18],[19],[20],[21],[22],[23] In our study too, 6-month overall survival in patients treated by whole brain radiation was 50.72% as compared to 66.67% in limited field radiotherapy and this difference was not statistically significant. According to Chouchair et al, the outcome of patients was similar with limited volume irradiation (LVI) as compared to patients treated with whole brain irradiation (WBI).[9] Patients treated with WBI had an average survival time of 8.2 months compared to 20.4 months in patients treated with localized field. The review of all the available autopsy material in the study revealed that in those patients where the tumor persisted, it was within the treated volume. Therefore, it is evident that recurrence is related to the resistance of the tumor itself rather than a geographic miss. The major obstacle to the delivery of radiation doses higher than 60 Gy has been the normal brain tissue tolerance. Late radiation damage is related not only to the total dose of radiation and dose per fraction but also to the volume of normal brain irradiation.[5] The recommendation on the adequate prescription of planning target volumes, however, varies considerably between various studies.[24]-[26] A precisely delineated target volume and planning treatment volume (PTV) (including 2 cm beyond the typical enhancing rim of high-grade glioma as demonstrated on the preoperative CT examination) seem to be more appropriate but have a recurrence rate of 90%.[14],[26] The PTV prescribed in our study included gross tumor volume plus a 3-cm margin beyond the enhancing rim of the high-grade glioma as demonstrated on the preoperative CT/MRI scan. Various studies have been conducted for examining the pattern of treatment failure in high-grade gliomas.[11],[15] Hochberg and Pruitt[11] studied the regrowth pattern for 62 malignant gliomas with respect to the area of tumor resection after treatment with whole brain irradiation (45Gy) and an external beam boost (15Gy). Fifty-nine of the patients (95%) had regrowth of tumor either within the resected area, or diffuse enlargement of the tumor at the primary site. Regrowth at a site away from the tumor bed was seen in only 3 of the 62 patients (5%). Wallner et al[15] studied patterns of treatment failure for 24 unifocal GBM and 8 unifocal anaplastic astrocytomas treated with whole brain radiotherapy with or without an external beam radiotherapy boost. Measuring the maximum distance between the edge of the recurrence and the edge of the initial tumor, they found that 56% of tumors (18/32) were confined to within 1 cm, 78% (25/32) within 2 cm, and 94% (30/32) to within 3 cm of the pre-surgical tumor margin. Only one patient (3%) had a recurrence which was distant from the primary tumor site. Gaspar et al[25] analyzed the site of failure with respect to teletherapy boost fields in 53 patients with malignant gliomas who failed after treatment with whole brain radiation therapy (44 Gy in 22 fractions) and an external beam boost (14 Gy in eight fractions). Failures were within the boost field in 38 (72%), partly outside the boost in 12 (23%), and totally outside the boost in 1 (2%) patient. Garden et al[24] observed disease progression in 34 out of 45 patients with malignant gliomas who received limited-volume external beam radiotherapy. Liang et al[26] studied the pattern of tumor recurrence in 10 patients with Grade 3 astrocytomas and in 32 patients with Grade 4 astrocytomas treated with external beam radiotherapy consisting of 45 Gy to the CT-defined tumor with a 3-cm margin followed by a 15Gy boost to the tumor with a 1.5-cm margin. The initial site of tumor recurrence was within a 2-cm margin of the original tumor. In our study too the majority of the tumor regrowths were within the original tumor volume. Three out of 12 in the study group and 5 out of 9 in the control group who had complete response, developed regrowth within a 2-cm distance of the initial gross tumor volume of contrast enhancement as seen on imaging. Only 1 patient in the study group had regrowth at a distance of more than 3 cm from the primary tumor margin. Thus from the majority of studies reported in the literature and from our study, there has been no survival advantage for local irradiation over whole brain irradiation. In patients with GBM and high-grade glioma, the survival duration is short hence it is important to at least try and improve the quality of life of these patients. An important finding in our study was that the performance status was markedly improved in those patients treated with limited field radiotherapy as compared to whole brain irradiation (80% vs. 56%). This difference was statistically significant. Conclusions There is no statistically significant difference in local control or overall survival between patients treated with whole brain irradiation and localized field irradiation. However, the KPS improved in more patients treated with localized field as compared to whole brain irradiation. In a disease like high-grade glioma when the overall survival is limited, this improvement in the quality of life attains significance. Hence we recommend limited field irradiation with a 3-cm margin around the enhancing tumor rim to a dose of 50 Gy to be followed by a boost to a 1.5-cm margin to a total dose of 60 Gy for patients with high-grade glioma. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=512;epage=517;aulast=Sharma The following images related to this document are available:Photo images[ni03164f2b.jpg] [ni03164t3.jpg] [ni03164t1.jpg] [ni03164f2a.jpg] [ni03164t2.jpg] [ni03164f3b.jpg] [ni03164f1.jpg] [ni03164t4.jpg] [ni03164f3a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}