 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
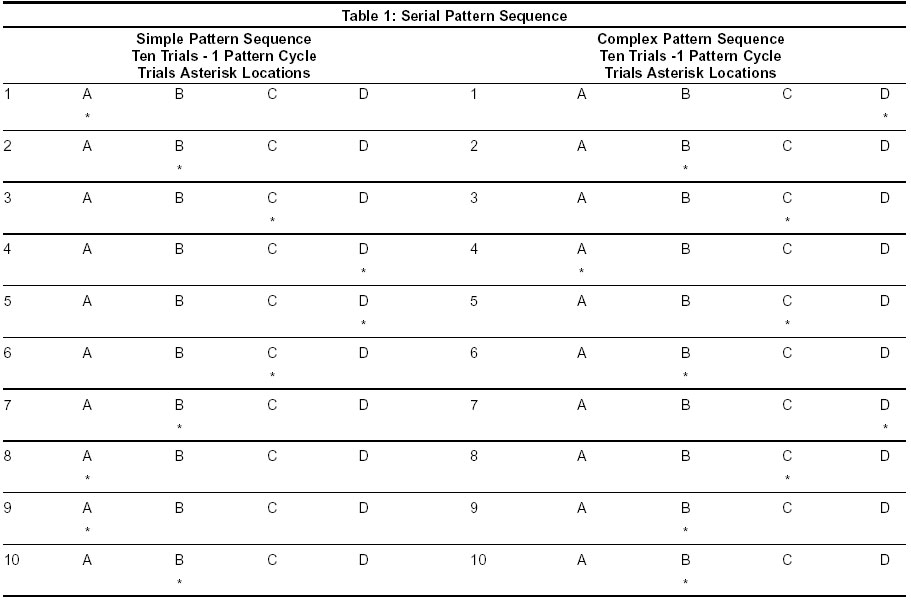
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 518-521 Original Article Serial pattern learning after mild head injury Shanmukhi S, Panigrahi M Clinical Psychologist, Deptartment of Neurology, Care Hospital, Hyderabad - 500001 Code Number: ni03165 Abstract Non-verbal serial pattern learning in patients with mild brain injury was examined using a serial pattern-learning task introduced by Nissen and her colleagues. The task involves two types of pattern cycles: Simple and Complex. Each pattern cycle consists of eight acquisition trials followed by a final generation phase, i.e. the ninth trial. The subjects responded to the asterisks appearing in repetitions of a 10-element spatial sequence in each pattern cycle. Eighty subjects were taken, of which 40 subjects had mild head injury and 40 were uninjured. Prior research with this task has shown that individuals show intact performance on the indirect measure of pattern learning, but are impaired on the direct measure. The results of this study showed that mild brain injury does cause a marked disruption in the ability to learn and remember serial pattern information in both simple and complex patterns.Introduction Interest in minor head injury has existed for some time, owing to its high rate of incidence and the relatively high morbidity associated with it. A major research focus of the past was on the post-concussional symptoms and why they persisted in some cases. There has been a strong interest in neuropsychological consequences based on the belief and hope that they would provide objective evidence of impaired brain functions. Significant impairment of neuropsychological functions, in the absence of other positive neurological findings, do in fact seem to occur within days of minor head injury. There is extensive literature showing that head injury leads to significant impairment in learning and memory.[1] For the most part, however, this research has focused on memory for verbal information (e.g. words, paired associates, and sentences). Only a few studies have addressed the question of whether the memory impairment associated with head injury extends to non-verbal information.[2],[3],[4],[5],[6] Rimel et al[7] published an exhaustive analysis on 538 patients. With mild head injury defined on the basis of the following parameters: loss of consciousness for less than 20 minutes, Glasgow coma scale (GCS) values ranging between 13 and 15, length of hospitalization less than 48 hours, follow-up was performed on 424 patients 3 months after the trauma; of these 79% complained of persistent headaches 59% had memory loss, and 34% had not resumed occupational activities. Synthesis of the neurobehavioral studies to date of patients with mild head injury indicates that (1) Cognitive problems are pervasive during the first week following injury; (2) These sequelae tend to resolve in 1-3 months, at least as judged by clinical neuropsychological measures; and (3) Subjective symptoms such as headache, fatigue and dizziness may persist for 3 months or longer. The memory disorder associated with head injury and many other types of brain damage seems to be restricted to direct tests of memory. However, the few prior studies of memory for non-verbal information after head injury have not examined performance on both direct and indirect tests. Brooks and his colleagues used a continuous recognition test to assess head injury patients' memory for visuospatial designs.[2],[3],[4] In these experiments, patients were shown a set of nonsense and geometric designs, some of which were repeated on later trials, and were asked to identify the designs as either 'new' or 'old'. Hannay et al,[6] used a similar continuos recognition task, but presented line drawings of familiar objects as stimuli rather than the unfamiliar designs used by Brooks et al.[5] These studies indicated that head injury produces slower learning rates, and lowers recognition scores for visuospatial materials.[2],[3],[4] Other studies have shown that head injured patients' ability to reproduce the complex Rey figure is also impaired, although they apparently have little difficulty reproducing very simple geometric designs.[2] Since the memory measures in these studies involve deliberate recollection, a reasonable assumption is that head injury lowers performance on direct tests of non-verbal memory. In the experiment reported here, we investigated the effects of head injury on the acquisition and retention of serial pattern learning within two weeks of trauma in patients with mild head injuries. We used a task introduced by Nissen and her colleagues.[8],[9],[10],[11] The serial learning task used in the present research offers both direct and indirect measures of non-verbal memory. Responding in the acquisition phase of this task does not require recollection of the pattern and therefore provides an indirect measure of memory for the pattern. Accurate prediction in the generation phase does require recollection of pattern knowledge and thus affords a direct test of memory for the pattern. The evidence that head injury leads to impairment on direct, but not indirect tests of memory for verbal information, combined with the fact that it also produces substantial deficits on direct tests of memory for non-verbal information led us to expect that our head-injured patients would display normal memory for the pattern in the indirect acquisition phase of the serial learning task, but would perform worse than control subjects in predicting the location of asterisks in the “direct” generation phase of this task.[2],[3],[4],[6],[12] Material and Methods Subjects (1) Glasgow coma scale (GCS) ranging from 13-15 (with a maximum score
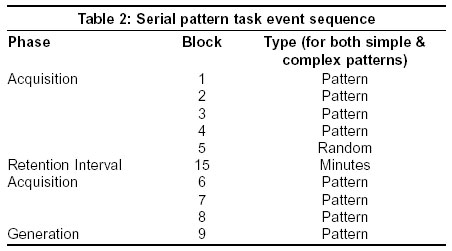
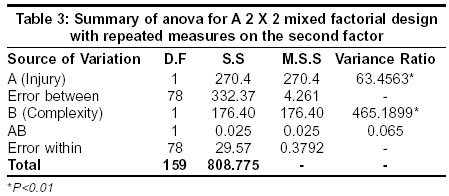
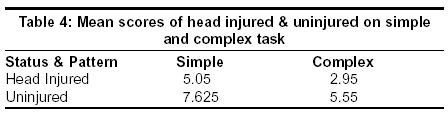
of 15). Teasdale and Jennett[13] introduced the GCS, i.e. the Glasgow coma scale in 1974. The primary distinction between moderate and mild head injury has been the sum score of 9-12 for moderate injury, and 13-15 for mild injury. Post-traumatic amnesia (PTA) of the patient was also checked as it helps in assessing the severity of the injury; the duration of PTA is the most sensitive and reliable index of severity for cases without signs of focal damage. The performance of the head injury patients was compared with that of an appropriately matched control group. The control group consisted of 40 volunteers who were relatives or friends of the patient, who had no history of prior head injury, alcoholism, drug intake, epilepsy, cerebral disease, mental retardation or significant psychiatric disorder and matched the patients in terms of age (20-40), educational qualifications (7th standard) and socio-economic background. Procedure Three additional pattern blocks were given after the random block and these were followed in turn, by the generation phase. And all blocks were separated by a rest period of at least 2 minutes, with the exception of blocks 5 and 6, which were separated by 15 minutes retention interval. During this interval, subjects did unrelated filler tasks and took a short break. The sequence of locations in the serial pattern and the sequence of events that occurred during the serial learning task in the simple and complex patterns are shown in [Table - 1] & [Table - 2]. Results For each subject, the correct responses of the generation phase were noted in the simple and complex pattern of the study group (head injured) and matched the control group (uninjured). The significance of the difference between the two groups was computed by using ANOVA. The obtained F values of 63.4563 for Factor A (the factor of injury) and 465.1899 for Factor B (the factor of complexity of the task) are significant at 0.01 level which is shown in [Table - 3]. The difference in the mean scores, both simple and complex, between head injured subjects (5.05 & 2.95) and uninjured subjects (7.625 & 5.55) show significant differences in learning and remembering. This is evident in [Table - 4]. Thus, it is seen that the head injured subjects had marked disruption in their ability to learn and remember in serial pattern learning (both simple and complex pattern). Further, there is a significant difference in terms of disruption in the learning and remembering of simple and complex patterns between the uninjured and head injured subjects. In simple terms, people with head injury find it more difficult to learn the complex pattern, however, uninjured people also experience a difference in learning the complex pattern to the same extent as the head injured. This is strongly supported by the high F value of 465.1899 with 1 d.f width, which is highly significant beyond 0.01 levels. The interaction (A*B) F value is 0.0659, which goes to show that there is no interaction effect. Discussion It has to be noted that memory loss is a common and core symptom of traumatic brain damage. The interest in PTA is obvious. According to Brook, PTA is defined as the interval between injury and regaining continuous day-to-day memory with intact orientation.[2] This investigation has helped to study the retrieval process. Neurophysicians generally assess PTA by questioning the patient about noticeable events in the hospital. It is generally conceded that attention influences memory, and subjective organization is an important part of memory. Sternberg and Tulving[14] have demonstrated that memory performance in normal subjects is related to the amount of “subjective organization” that they apply to the material to be learned. Information would be better recalled, the more the operations a subject has carried out on it, e.g. by grouping items into clusters, or by noting similarities between the items. Again, the mental slowness of the head injured patient reduces his capacity to organize the material subjectively as he can do less in certain time units than his healthy counterpart. In this study, it may be pointed out that this temporary inability to organize partly explains the poor results of patients in a task in which non-verbal information has to be learned. In this task, the acquisition phase of the serial learning task reflects the operation of procedural memory, whereas the generation phase reflects the operation of declarative memory. In agreement with this idea, we believe that “procedural learning” is an apt characterization of the type of learning that occurs during the acquisition phase of the serial learning task. It was observed in this study that the severity of injury is associated with slowing down in the rate of acquisition of pattern information, which supports the conclusion that head injury can lead to deficits in procedural learning. This fact is supported by Nissen et al[10] and Willingham et al.[15] In conclusion it could be suggested on the basis of this study that the the present kind of investigation would go a long way in the cognitive assessment and rehabilitation of the patients. It is significant to note that non-verbal material confined to a simple task used in this study presumably could lessen the strain of organizing the material in the patients. At the same time, it will also yield data, which can be gainfully employed in the early rehabilitation of patients. This assumption is in consonance with the findings of those who found that 251 hospitalized patients with mild head injury recovered in an average of 17.7 days with psychological assistance against a control group of patients hospitalized but without active rehabilitation, who recovered only after 32.2 days.[16] Gradual resumption of work or school activities, advice for stress management and return for a brief follow-up examination (which includes assessment of cognitive functioning) 2-4 weeks after discharge are recommended for patients sustaining a mild head injury. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=518;epage=521;aulast=Shanmukhi The following images related to this document are available:Photo images[ni03165t2.jpg] [ni03165t1.jpg] [ni03165t4.jpg] [ni03165t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}