 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
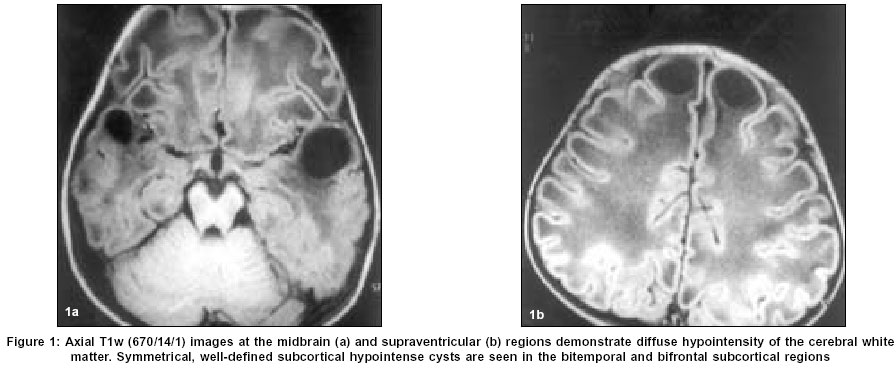
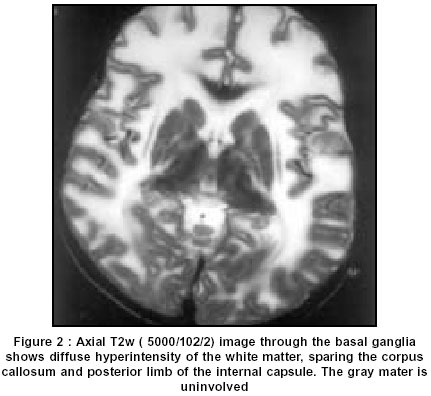
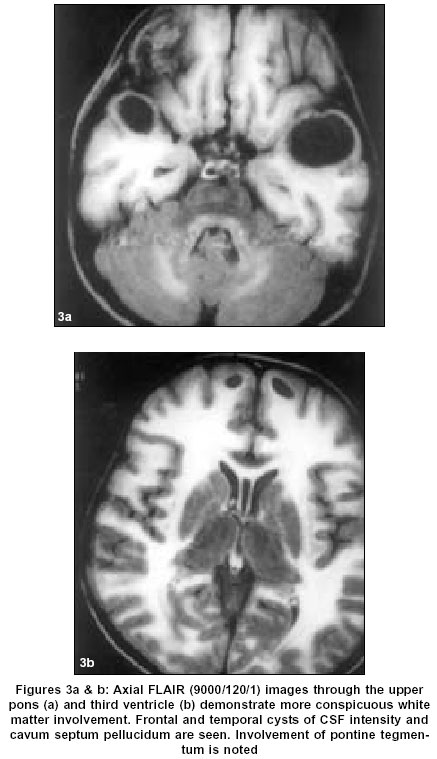
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 525-527 Case Report Megalencephalic leukoencephalopathy with subcortical cysts: MRI and proton spectroscopic features Chandrashekar HS, Guruprasad AS, Jayakumar PN, Srikanth SG, Taly AB Departments of Neuroimaging and Interventional Radiology, National Institute of Mental Health and Neuro Sciences, Bangalore - 560029 Code Number: ni03167 Abstract Megalencephalic leukoencephalopathy with subcortical cysts (MLC) is a rare, recently described disease.1 This disorder, reported predominantly in infants and children, was originally described by van der Knaap as ‘leukoencephalopathy with swelling and a discrepantly mild clinical course’. The gene locus for this autosomal recessive disease has been assigned to chromosome 22qtel, and a gene has been identified, presently called MLC1.2,3 It is characterized clinically by a large head and mild neurological symptoms such as ataxia, spasticity and remarkably slow course of functional deterioration. The MRI features described include ‘swollen white matter’ with large symmetrical cystic changes in the cerebral hemispheres.1,2,4 The MRS findings in this disorder include mild to moderate decreases in the NAA to choline and choline to creatine ratios.5 We report a child with this disease and discuss the MRI and MRS features. Introduction Megalencephalic leukoencephalopathy with subcortical cysts (MLC) is a rare, recently described disease.[1] This disorder, reported predominantly in infants and children, was originally described by van der Knaap as 'leukoencephalopathy with swelling and a discrepantly mild clinical course'. The gene locus for this autosomal recessive disease has been assigned to chromosome 22qtel, and a gene has been identified, presently called MLC1.[2],[3] It is characterized clinically by a large head and mild neurological symptoms such as ataxia, spasticity and remarkably slow course of functional deterioration. The MRI features described include 'swollen white matter' with large symmetrical cystic changes in the cerebral hemispheres.[1],[2],[4] The MRS findings in this disorder include mild to moderate decreases in the NAA to choline and choline to creatine ratios.[5] We report a child with this disease and discuss the MRI and MRS features. Case Report A 25-month-old boy, second sibling of a non-consanguineous marriage, was admitted with symptoms of delay in speech acquirement and inability to walk without support. The child had a big head since birth but the acquisition of motor milestones in infancy was normal. The child had frequent falls. There was no history of seizures or of visual disturbances. His head circumference was 54.5 cm. The reflexes were brisk in the lower limbs with bilateral extensor plantar responses. On Vincland Social Maturity Scale (VSMS), the child had a normal level of social functioning and on Gessel's Children Behavior Schedule, mild delay in language functions and personal social behavior. No other abnormality was detected clinically. Urine analysis for inborn errors of metabolism and metachromatic granules was negative. EEG and ENMG were normal. MRI and in-vivo MRS were performed on a 1.5T superconducting system. The MR features were strikingly abnormal with diffuse involvement of the cerebral white matter. On T1w images, the involved white matter was hypointense and had a characteristic 'swollen' appearance, with obliteration of the sulci [Figure:1a] & [Figure:1b]. On proton-density, T2w and FLAIR sequences, these areas were hyperintense. The peripheral and periventricular white matter were equally involved with sparing of some central white matter structures like the corpus callosum, anterior limb of the internal capsule and bilateral posterior occipital radiations [Figure - 2]. Minimal hyperintensity of the long tracts of the mesencephalon was noted. The cortical and central gray matter and the cerebellum were uninvolved [Figure:3a]. Large, well-defined, oval cystic lesions, which followed CSF intensity on all sequences, were seen symmetrically in subcortical locations of bifrontal and bitemporal poles and in the left parietal lobe [Figure:3a]. Cavum septum pellucidum and cavum vergae were noted [Figure:3b]. The ventricular system was unremarkable. In-vivo localized multi-voxel proton spectroscopy was performed [Hybrid 2D Chemical Shift Imaging (2DCSI); TE=135 ms] from the involved corona radiata and normal-appearing basal ganglia. The spectra showed minimal reduction in the NAA/ choline and NAA/ creatine ratios [Figure:4]. Discussion The combination of megalencephaly and leukoencephalopathy is seen in a limited number of disorders. The characteristic swollen white matter changes, as seen on MRI, have only been reported in MLC,[1],[4] Canavan's disease,[6] Alexander's disease,[7] L-2-hydroxyglutaric aciduria,[8] and one variant of congenital muscular dystrophy.[9] Our patient fulfills the imaging criteria for MLC[1]. In Canavan's disease, MRI shows additional involvement of the thalamus and globus pallidus, and increased NAA content on 1H MRS.[10] NAA was normal in our patient. In Alexander's disease, contrast enhancement of the periventricular region, caudate nuclei and thalami, frequent presence of hydrocephalus and often, prominent cavitation in the frontal periventricular white matter are characteristic features.[7] None of these were observed in our patient. Also, Alexander's disease with infantile onset is a much more severe condition with early death. In L-2-hydroxyglutaric aciduria patients, the involvement of dentate nuclei and severe atrophy of cerebellar vermis are additional features.[8] The cerebellum was uninvolved in our patient. Sphingolipidoses, mucopolysaccharidoses, type 1 glutaric aciduria lack the characteristic 'white matter swelling'.[1] In a series of 8 patients with MLC described by van der Knaap, the supratentorial deep white matter was diffusely involved and swollen in all the patients. All patients had typical subcortical cysts in the anterior temporal and/or frontoparietal regions. Cavum septum pellucidi and cavum vergae were seen in all patients. The pyramidal tracts in the brainstem were involved in 3 patients with 'slight' involvement of the cerebellar white matter in 6 patients.[1] van der Knaap described the histological findings in a 13-year-old boy with MLC.[11] It revealed cavitating spongiform leukoencephalopathy with vacuoles in the outermost lamellae of myelin sheaths. Subcortical white matter showed intense fibrillary astrogliosis. Myelinated axons and cortical neuronal structures were preserved.[11] The MRS features in our patient corroborate those histopathological features with no appreciable neuronal loss (near normal NAA), no demyelination (no increase in choline) and absence of gliosis (normal mI). The spectra from the basal ganglia were normal. Another MRS report of a severely affected 8-year-old child with MLC showed loss of all metabolites.[12] Decreased NAA/Cr ratios have also been reported in adult patients with MLC.[5],[13] A milder clinical course is associated with less severe metabolic changes.[13] While an Asian Indian ethnic group in which MLC is particularly prevalent has been identified,[14] our patient is not from that ethnic group. MLC should be considered in the differential diagnosis of children with megalencephaly and leukoencephalopathy. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=525;epage=527;aulast=Chandrashekar The following images related to this document are available:Photo images[ni03167f3ab.jpg] [ni03167f2.jpg] [ni03167f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}