 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
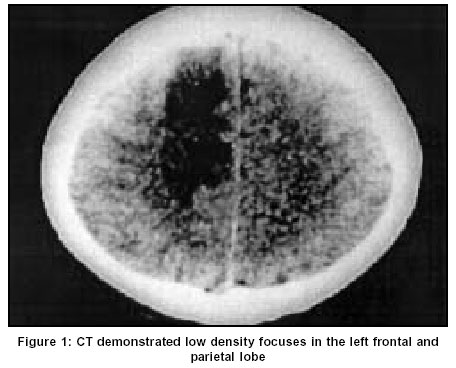
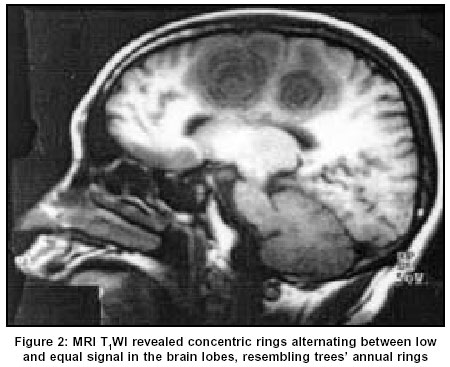
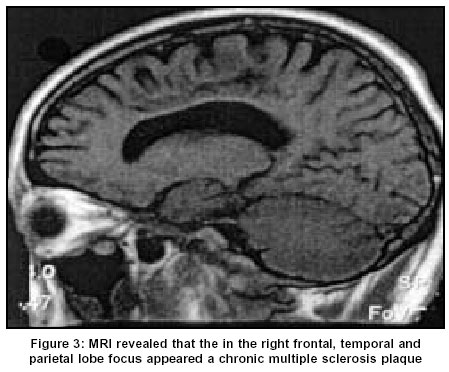
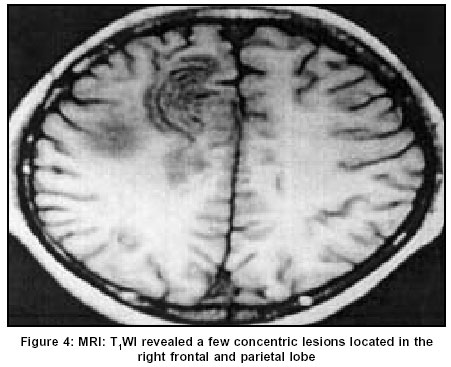
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 528-530 Case Report Concentric sclerosis: Imaging diagnosis and clinical analysis of 3 cases Gu J, Wang R, Lin J, Fang S Institute of Biomedical Engineering of the Huazhong University of Science and Technology, 1037 Luoyu Ave, Wuhan, 430074 Code Number: ni03168 Abstract Baló’s Concentric sclerosis (BCS) is a rare demyelinating disease considered to be a variant of multiple sclerosis (MS). The typical magnetic resonance imaging (MRI) changes associated with BCS consist of concentric rings or onions’ cross-section on T1-weighted (T1W) images. Because MRI reveals pathological changes consistent with autopsy in the focus of BCS, it plays an important role in the before-death diagnosis of BCS. We report three cases of BCS diagnosed antemortem on the basis of the typical concentric rings pattern on MRI and on the basis of clinical findings and cerebrospinal fluid (CSF) examination. BCS often occurs in the prime of life, acutely or subacutely. Then come cerebral multifocal symptoms and signs. We find that BCS is not always an acute and irreversible pathological process as described in the past.Introduction Baló's Concentric sclerosis (BCS) is a rare demyelinating disease considered to be a variant of multiple sclerosis (MS).[1] The characteristic pathological findings are alternating rings of myelin preservation or remyelination and myelin loss, which appear as concentric pattern streaks alternating between light and shade, resembling trees' annual rings or onions' cross-section.[2],[3] Less than 60 cases have been reported in the literature.[3] Our 2 case reports support the concept that BCS may be a self-limiting disease that is not always fatal and the MRI appearance of the chronic lesion may resemble that of a chronic MS plaque.[3],[4],[5] Characteristic MRI findings may allow antemortem diagnosis of BCS when performed at the onset of the disease.[6],[7] Case Report Case 1 Reinforced MRI scan revealed distinct incomplete rings reinforcement in the right temporal lobe. After 1 month, MRI scan revealed the following: the focus in the above-mentioned lobe. became smaller; and concentric rings were visible on T2W and T1W. CSF examination disclosed a normal routine and biochemical, negative oligoclonal bands. Dexamethasone (15 mg/day) was IV administered for 15 days, and the patient's condition improved within a few days. Three weeks later, the results of the patient's neurological examination revealed muscle power of the left upper and lower limbs recovered to MRC grade 5/6 and 4/6 respectively. During 3 years of follow-up, there were no further relapses. Half a year later, MRI revealed that the focus decreased remarkably (diameter: 1-2 cm). Final MRI, performed approximately 3 years after the first attack, showed that the concentric pattern had completely disappeared and that only a small, residual non-specific, gliotic, plaque-like lesion remained. No additional lesion was detected [Figure - 3]. Case 2 Case 3 Discussion The group of 3 cases observed were diagnosed as BCS, based on the characteristic concentric rings found on MRI and clinical findings. Kim Mo[7] and Boloy's[5] hold that the etiological factor of BCS is possibly the same as that of MS. Currently, the common viewpoint is that BCS is a variation of MS. Yao[8] holds that, in its pathogenesis, the loss of oligodendrocytes plays an important role in the demyelination. The courses of Cases 1 and 3 were longer and the prognosis was good in the 3 cases, which is different from the Weinshenker BG[2] reports while consistent with Boloy's findings.[5] In all the 3 cases, the CT-proposed diagnosis was cerebral infarction, brain tumor, brain abscess, inflammatory granuloma, etc.; MRI, especially T[1]WI, revealed concentric patterns alternating between low and equal signal in white matter, resembling onions' cross-section; it was even more distinct with Gd-DTPA. In past diagnosis of BCS was mainly based on autopsy.[7],[9] Currently, besides the biopsy of brain, MRI is the main diagnostic means for BCS before death[6] as MRI reveals pathological changes consistent with autopsy in the focus of BCS.[6],[9],[10],[11] The combination of proton magnetic resonance spectroscopy (1H-MRS) and the typical MRI revelation suggested by Kim[7] and Ercan Karaarslan[3] may take the place of brain biopsy in the diagnosis of BCS when performed at the onset of the disease. Early treatment with sufficient glucocorticoid can remit clinical symptoms.[3] The 3 cases were all treated with Dexamethasone 15 mg for 10-15 days. The clinical symptoms of two cases got a relatively long period of remission. The patients did not experience any relapse for 1-and-a-half to 3 years. As to the prognosis of BCS, previous reports included an extremely dangerous state, short course, quick progress to death with a survival period ranging from several weeks to months.[2] However, according to the cases diagnosed antemortem by biopsy of brain or MRI in recent years,[2],[3],[4] although the onset of illness is acute and the patient's condition is serious, the clinical symptoms of patients remit partially or disappear completely after timely treatment, which is consistent with our Cases 1 and 3. This suggests that Balo's disease is not always an acute and irreversible pathological process as described in the past. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=528;epage=530;aulast=Gu The following images related to this document are available:Photo images[ni03168f1.jpg] [ni03168f4.jpg] [ni03168f3.jpg] [ni03168f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}