
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 51, Num. 4, 2003, pp. 534-536
|
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 534-536
Case Report
Delayed pharyngo-esophageal perforation: Rare complication of anterior cervical spine surgery - Case reports
Shenoy SN, Raja A
Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal
Correspondence Address:Department of Neurosurgery, Kasturba Medical College
and Hospital, Manipal - 576119. Udupi, shenoysn@yahoo.com
Code Number: ni03170
Abstract
An injury to the pharynx and esophagus is a known complication of anterior cervical spine surgery. Two cases of delayed pharyngo-esophageal perforation following anterior cervical spine surgery that resulted in fistula are presented. We postulate that graft displacement and dislodgement of implant with resulting esophageal erosion was responsible for this complication.
Introduction
Injuries to the pharynx and esophagus are known complications of anterior
cervical spine surgery.[1] One-third
of the reported cases of esophageal perforation occurred during surgery.[1] Very
few cases of delayed pharyngo-esophageal perforation are reported
in the literature.[1],[2],[3],[4],[5] Of
the 260 cases of anterior cervical spine surgeries in the last 15
years, we had 2 cases of delayed esophageal fistulas. We report these
cases of delayed pharyngo-esophageal perforation secondary to anterior
cervical spine surgery.
Case Reports
Case 1
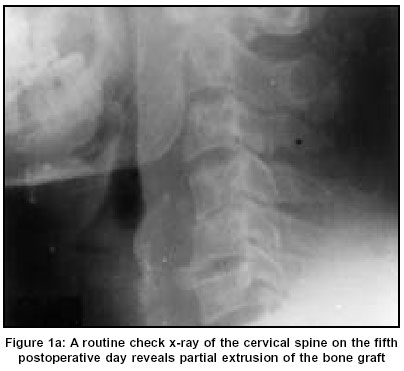
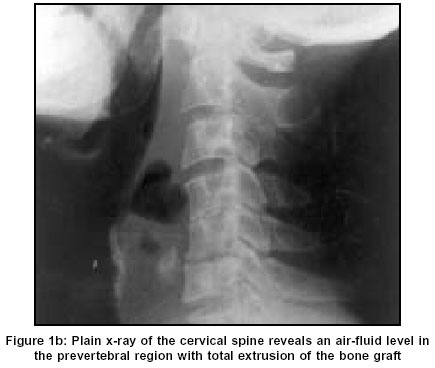
A 32-year-old gentleman underwent discectomy at C4-5 and C5-6 levels with single level bony fusion for cervical myelo-radiculopathy. A routine check X-ray of the cervical spine on the 5th postoperative day revealed partial extrusion of the bone graft [Figure:1a]. As the patient was asymptomatic, he was treated conservatively with cervical collar and discharged. He presented to us again at the end of 4 weeks with history of sudden bouts of purulent vomiting and a progressively increasing swelling at the operation site. On examination, he had a diffuse tender swelling at the operation site. Plain X-ray of the cervical spine revealed an air-fluid level in the prevertebral region with total extrusion of the bone graft [Figure:1b]. While he was waiting for drainage, the swelling ruptured discharging purulent material containing mucus and food particles. He underwent drainage of the pus and debridement including removal of the extruded bone graft. The culture of the pus showed growth of mixed organisms with sensitivity to multiple antibiotics. Hence he was started on Inj. Penicillin, Chloromycetin and Metronidazole. Postoperatively, he was continued on antibiotics and Ryle's tube feeding for 4 weeks. At 4-year follow-up, the patient was asymptomatic and X-ray of the cervical spine revealed bony fusion and no evidence of instability.
Case 2
An 18-year-old gentleman was referred to our department, with history
of discharge from the neck. He underwent anterior cervical stabilization
using plate and screw for fracture of the C4 vertebra [Figure:2a].
About 3 weeks later he developed a swelling at the operation site,
which later ruptured discharging pus and food materials. On neurological
examination, he was quadriplegic with grade 0/5 power below C6 level.
The fistula was diagnosed after confirming the leakage of oral methylene
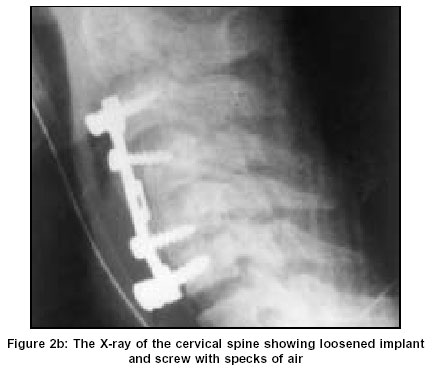
blue from the operated site. The X-ray of the cervical spine showed
loosened implant and screw with specks of air [Figure:2b]. He underwent
drainage of the pus and debridement. The implant was found loose
and eroding into the esophagus causing a large defect in the posterior
esophageal wall. As the edges of the defect were edematous and friable,
primary closure of the defect could not be done. Hence the sternocleidomastoid
muscle flap was used to repair the esophageal defect. The pus culture
showed growth of the Staph. Epidermidis sensitive to penicillin,
quinolones, vancomycin and amino glycosides. Postoperatively, the
patient was continued on Ryle's tube feeding and antibiotics (Penicillin
and Gentamycin) for 8 weeks. Despite external healing of the fistula,
esophagogram revealed persistent extravasation of contrast at the
end of 3 weeks [Figure:2c]. Hence tube feeding was continued for
one more month before starting oral feeding. At 6-month follow-up,
in spite of complete healing of fistula, there was no change in his
neurological state. The patient expired 2 months after the follow-up
due to renal failure.
Discussion
Esophageal perforation following anterior cervical spine surgery is an uncommon but potentially devastating complication.[1],[2] This complication may occur during surgery, early in the postoperative period or months later.[2] Very few cases of delayed esophageal perforation are reported in the literature.[1],[2],[3],[4],[5] As it has happened in the present cases, the esophageal perforation is commonly associated with protruded or loosened hardware or dislodged bone graft.[1] Persistent dysphagia, especially associated with odynophagia following anterior cervical spine surgery should be evaluated for graft/implant-related complications.[6] The presence of air in the fascial planes of the neck and increasing soft tissue swelling in the postoperative X-ray suggest esophageal perforation.[6] The diagnosis can be confirmed by contrast esophagography with a high accuracy rate.[1],[5]
The treatment of esophageal perforation depends upon the severity of the problem, the patient's general condition and the presence of any complications. Asymptomatic extrusion of the graft in the gastrointestinal tract should be observed carefully for the development of any complications.[3],[4],[7] Patients presenting with external fistula and abscess formation require wound debridement and removal of the graft and internal fixation device as described in our patients.[2] Patients with a large esophageal defect require reinforcement using the sternocleidomastoid muscle flap.[8] It is better to delay oral feeding for at least 4-6 weeks after the healing is demonstrated radiologically.[5] We conclude that graft/implant dislodgement was responsible for the esophageal perforation, and early recognition and proper management of postoperative esophageal fistulas prevents further major complications.
References
| 1. | Newhouse KE, Lindsey RW, Clark CR, Lieponis J, Murphy J. Oesophageal perforation following anterior cervical spine injury. Spine 1989;14:1051-3. Back to cited text no. 1 |
| 2. | Guyer RD, Delamarter RB, Fulp T, Small SD. Complication of cervical spine injury In: Rothman - Simeone. The spine Ed 4, Philadelphia: WB Saunders; 1999. pp. 540-52. Back to cited text no. 2 |
| 3. | Sharma RR, Sethu AU, Lad SD, Turel KE, Pawar SJ. Pharyngeal perforation and spontaneous extrusion of the cervical graft with its fixation device: a late complication of C2-C3 fusion via anterior approach. J Clin Neurosci 2001;8:464-8. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Geyer TE, Foy MA. Oral extrusion of a screw after anterior cervical spine plating. Spine 2001;26:1814-6. Back to cited text no. 4 [PUBMED] [FULLTEXT] |
| 5. | Jamjoom ZA. Pharyngo-cutaneous fistula following anterior cervical fusion. Br J Neurosurg 1997;11:69-74. Back to cited text no. 5 [PUBMED] |
| 6. | Loop FD, Groves LK. Collective Review, Oesophageal perforations. Ann Thorac Surg 1970;10:571-87. Back to cited text no. 6 [PUBMED] |
| 7. | Pompili A, Canitano S, Caroli F, Caterino M, Crecco M, Raus L, et al. Spine 2002;27:E499-E502. Back to cited text no. 7 |
| 8. | Fuji T, Kuratsu S, Shirasaki N, Harada T, Tatsumi Y, Satani M, et al. Oesophagocutaneous fistula after anterior cervical spine surgery and successful treatment using a sternocleidomastoid muscle flap. A case report. Clin Orthop 1991;267:8-13. Back to cited text no. 8 |
Copyright 2003 - Neurology India Free full text also available from:
http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=534;epage=536;aulast=Shenoy
The following images related to this document are available:
Photo images
[ni03170f1b.jpg]
[ni03170f1a.jpg]
[ni03170f2c.jpg]
[ni03170f2b.jpg]
[ni03170f2a.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}