 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
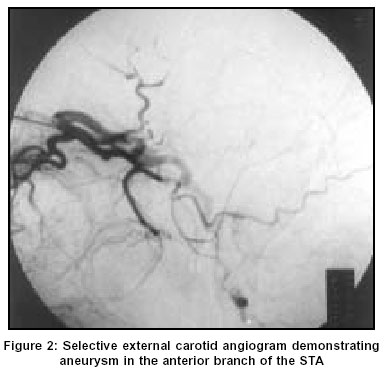
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 537-538 Case Report Traumatic superficial temporal artery aneurysm: Case report Shenoy SN, Raja A Department of Neurosurgery, Kasturba Medical College & Hospital, Manipal Code Number: ni03171 Abstract Traumatic aneurysm of the superficial temporal artery is an uncommon lesion. Two cases of post-traumatic superficial temporal artery aneurysm are presented. Introduction Aneurysms of the superficial temporal artery (STA) are uncommon with less then 200 cases reported in the literature.[1],[2],[3],[4],[5] Usually, these aneurysms are false aneurysms and occur following blunt or penetrating trauma to the head or following surgery in the temporal region.[6],[7],[8],[9],[10],[11],[12] Most of these patients present within 2-6 weeks of injury.[7] In this report, we present 2 cases of STA aneurysm following a closed head injury. Case Report Case 1 He was investigated with selective external carotid angiography, which demonstrated an aneurysm arising from the anterior branch of the left superficial temporal artery [Figure - 2]. The aneurysm was exposed surgically and the proximal and distal artery were ligated and the aneurysm was excised. Case 2 On examination, he had a well-defined, non-tender, pulsatile swelling measuring 1.5 cm in diameter. The swelling decreased in size and became non-pulsatile on compressing the proximal anterior branch of the STA. A diagnosis of post-traumatic STA aneurysm was done. Due to the unwillingness of the patient to undergo any investigation, he was directly subjected to surgery. Under local anesthesia, a skin crease incision was made over the swelling and the aneurysm with both proximal and distal artery was exposed and ligated and excised. The postoperative period was uneventful. Discussion Aneurysm of the STA was first described by Bartholin in 1740.[8] More than 95% of aneurysms of the STA are traumatic in origin.[6],[7],[8],[9] The majority of these aneurysms were found in males.[6],[9],[12] These aneurysms are false aneurysms.[6],[7] A false aneurysm is defined as one in which the lumen is not surrounded by all the 3 layers of the arterial wall.[13] The STA, after originating from the external carotid artery at the base of the parotid gland runs through a relatively exposed course over the temporal bone.[1] Hence one might expect more injuries to the vessel than have been reported.[8] The mechanism of injury is either a partial transection of the artery or severe contusion and necrosis of a sector of the arterial wall.[1] The intact overlying skin confines the resultant hemorrhage. The hematoma becomes progressively organized so that a fibrous pseudocapsule forms and the artery may become recanalyzed. Thus, progressive lysis and resorption of luminal thrombus may permit substantial reflow through the vessel. Progressive dilation of the weak hematoma capsule explains the appearance of a pulsating mass.[8] The diagnosis of STA aneurysms can usually be made by history and physical examination. The usual presenting symptom is a pulsating swelling in the temporal region or a throbbing headache.[8] The mass is usually single and pulsatile in nature and on compression of the STA proximally, there will be a diminution or disappearance of pulsation.[7],[12],[14] However, multiple STA aneurysms can also be seen in the same patient.[8] Non-invasive as well as invasive modalities can be used to make the diagnosis of STA aneurysm.[1] The most accurate non-invasive modality to aid in the diagnosis is a duplex ultrasound scan of the lesion, which shows the native vessel with a fusiform dilatation consistent with the mass and the presence of turbulent intraluminal blood flow.[1] Computed tomographic [CT] scan with contrast has also proven useful in the diagnosis of STA aneurysm.[2],[15] Angiography not only confirms the diagnosis but also clarifies the feeding vessels.[8] We performed selective external carotid angiography in Case 1 and confirmed the diagnosis preoperatively. However, in Case 2, the diagnosis was made clinically and confirmed intraoperatively. Similarly, the literature supports the view that the diagnosis of STA aneurysms can be made by history and clinical examination alone and CT scan and angiography are unnecessary.[14],[16] The treatment of STA aneurysms varies from a conservative method such as repeated compression of the lesion to surgical excision of the lesion.[1],[7],[14],[17] A few cases of successful endovascular obliteration of the STA aneurysm are reported in the literature.[18],[19] The treatment of choice is excision of the aneurysm and ligation of the afferent and efferent vessel.[7],[8],[14] Even though in Case 1 the compression method was tried, there was no success. Hence surgical excision of the lesion was considered. Surgery is indicated to reduce the risk of hemorrhage from trauma, to relieve headache and to resolve the cosmetic defect.[8],[20] References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=537;epage=538;aulast=Shenoy The following images related to this document are available:Photo images[ni03171f1.jpg] [ni03171f2.jpg] |
| |||||||||

{kind=link}
{kind=link}