 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
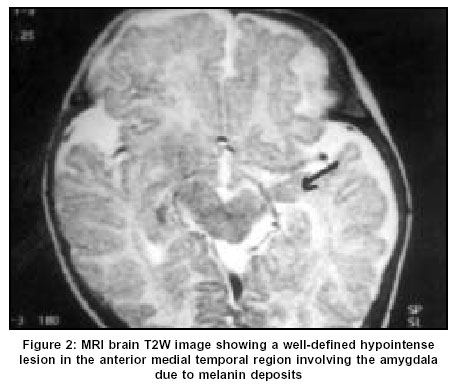
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 541-543 Case Report Multiple giant congenital melanocytic nevi with central nervous system melanosis: A case report Ahuja SR, Karande S, Kulkarni MV Division of Pediatric Neurology, Department of Pediatrics, L.T.M. Medical College and L.T.M.G. Hospital, Sion, Mumbai - 400022 Code Number: ni03173 Abstract A case of multiple giant congenital melanocytic naevi in whom central nervous system melanosis was detected at 6 weeks of age is described. The infant was asymptomatic, but presence of risk factors such as multiple naevi, giant naevi and naevi on scalp and posterior axial location prompted a magnetic resonance imaging study of the brain. To our knowledge, neurocutaneous melanosis at such a young age has not been reported in Indian literature.Introduction A congenital melanocytic nevus is defined as a melanocytic nevus present at birth or one which appears within first few months of life.[1] These naevi are classified into 3 types based on their final size; small (less than 1.5 cm in diameter), intermediate (1.5-20 cm in diameter), and giant or large (also called garment or bathing trunk nevi, measuring more than 20 cm in diameter). Allowing for expected proportionate growth, congenital melanocytic nevi measuring 6 cm or more on the body or 9 cm or more on the head in a neonate are labeled as giant congenital melanocytic nevi (GCMN).[2] GCMN is an uncommon birthmark occurring in approximately 1 in 20,000 live births.[3] We discuss a case of multiple GCMNs in whom asymptomatic central nervous system (CNS) melanosis was detected at 6 weeks of age.Case Report A 2-day-old male child, born to a primigravida by normal vaginal delivery, presented with multiple brownish-black patches all over the body. The largest patch covered nearly the entire back (17x13cm) and was smooth, flat and not covered by hair [Figure - 1]. The patch over the buttocks (11x5.5cm) was flat, covered with abundant hair and surrounded by smaller satellite lesions. The scalp showed another patch (7x5cm) with marked hypertrichosis. The birth weight was 3.2 kg, head circumference 33 cm and total body length 51 cm. His neurological examination was normal. MRI brain with contrast done at 6 weeks of age revealed a well-defined hyperintense lesion in the anterior medial temporal region involving amygdala on T1W images, which was hypointense on T2W images [Figure - 2]. Similar lesions were also seen in both thalami; more on the right than left. There was no mass effect, perilesional edema, abnormal leptomeningeal deposits or contrast enhancement. MRI spine was normal.Discussion GCMNs begin as flat, brown or brownish-black patches but with increasing age may become elevated and develop a mottled appearance and nodular surface.[1],[4] They appear darker at birth than a few weeks later and are found most commonly on the trunk, followed by the limbs and the head. The infant in the present case presented with 3 GCMNs viz. one each on scalp, back and buttocks. Giant naevi are almost always confined to the skin but rarely, invade underlying fascia and muscle.[5] Early and complete surgical excision is the recommended treatment for GCMN as they have an increased lifetime risk of malignancy viz. malignant melanoma and other neural crest malignancies.[1] The risk varies between 2-42%.[4],[6] A substantial percentage of these malignancies develop during childhood. Giant nevi on the scalp, in a posterior axial location and those with surrounding satellite nevi are at greatest risk of malignant transformation.[7],[8] The GCMNs in the present case were at greatest risk of malignant transformation. Abnormalities reported in association with GCMN are limb hypoplasia, ear deformities and angiomas.[6] The present case had no such associated abnormalities. More importantly, congenital melanocytic naevi may be associated with an increased number of melanocytes in the CNS, a phenomenon known as neurocutaneous melanosis (NCM).[9] In the CNS, melanocytes are normally present at certain sites viz. the reticular formation of the medulla and pons, in the substantia nigra and in the leptomeninges overlying the base of the brain.[9] NCM is believed to represent an error in the morphogenesis of embryonal neuro-ectoderm. In NCM, thick sheets of melanocytes are found in the pia, arachnoid, in the parenchyma of basal ganglia, dentate nucleus, pons, cerebellar hemispheres, thalamus and amygdala.[9] Almost all children with NCM have giant nevi on the head, neck or dorsal spine. The exact incidence of NCM and its outcome in otherwise asymptomatic persons with GCMN is not known. Till 1994, less than 60 cases had been reported.[6] Kadonaga and Freiden have laid down 3 risk factors for the development of CNS melanosis: a) giant or multiple (more than 3) naevi, b) no evidence of cutaneous melanoma, and c) presence of nevus/nevi on the scalp, neck or in the posterior axial location.[10] The present case had these risk factors for CNS melanosis which prompted us to do an MRI brain even though the infant was asymptomatic. In children with NCM, asymptomatic neurological status has been defined as normal achievement of milestones, normal head circumference and normal physical examination except for skin lesions.[10] NCM can cause neurological symptoms by causing abnormalities of circulation, resorption of CSF, local pressure effects or malignant transformation viz. CNS melanoma.[9] Most patients with CNS melanosis present in first two years of life with signs of raised intra-cranial pressure, seizures or spinal cord compression.[10] Symptomatic CNS melanosis, even in the absence of CNS melanoma, has an extremely poor prognosis.[10] CNS melanosis is best seen on MRI scan because the paramagnetic effect of melanin leads to a decrease in both T1 and T2 relaxation times with a highly characteristic appearance on imaging. The commonest finding is T1 shortening in the cerebellum, temporal lobes, pons and medulla.[1],[6] Knowledge of these locations helps to differentiate melanotic deposits which are part of the disease, from metastases secondary to malignant degeneration of a GCMN.[11] The advent of MRI has begun to change the perception of CNS abnormalities in patients with GCMN. It has become apparent that GCMN may be associated with various non-melanocytic CNS lesions like Dandy-Walker malformation,[12] encephalocele,[13] arachnoid cysts, Chiari type 1 malformation and intra-spinal lipomas.[6] In the present case, there were no associated non-melanocytic CNS lesions. Although CNS melanosis has no specific treatment at present, its detection alters the management of GCMNs. Its detection postpones the multiple surgical procedures required to remove the GCMNs since the melanin deposits in the CNS would still remain a source for malignant transformation viz. CNS melanoma.[6] A child with abnormality on initial MRI, as in the present case, must be examined at regular intervals for neurological signs; serial MRIs are recommended every 6 months to detect malignant transformation of CNS melanosis. Enlargement of a specific focus of T1 shortening or development of perilesional edema may warrant surgical exploration of the brain because early detection of a CNS malignant tumor could result in a surgically resectable tumor.[6] It is also important to remember that in a child with GCMN, a normal MRI brain study does not rule out the possibility of future occurrence of CNS melanosis. Thus serial MRIs are recommended in every child with GCMN who is at risk of developing CNS melanosis.[6] In the present case the GCMNs will be carefully observed for malignant transformation. If the child remains asymptomatic till his 5th birthday, plastic surgical interventions will be undertaken. To our knowledge, neurocutaneous melanosis at such a young age has not been reported in Indian literature. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=541;epage=543;aulast=Ahuja The following images related to this document are available:Photo images[ni03173f2.jpg] [ni03173f1.jpg] |
| |||||||||

{kind=link}
{kind=link}