 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
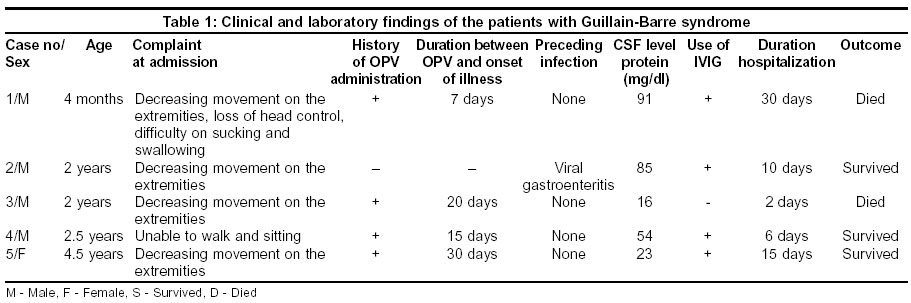
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 544-545 Case Report Report of five children with Guillain-Barré syndrome following a nationwide oral polio vaccine campaign in Turkey Anlar O, Tombul T, Arslan S, Akdeniz H, Caksen H, Gundem A, Akbayram S Department of Neurology, Yuzuncu Yil University Medical School, Van Code Number: ni03174 Abstract Five children with Guillain-Barre syndrome (GBS), following a national oral polio vaccination campaign to eradicate disease, are reported. Clinical examination, CSF and electromyographic findings conformed to the classical description of GBS. Four of them received therapeutic dose of intravenous IgG. Two children succumbed to the disease. It was observed that the number of cases of GBS in children increased during the period of the oral polio vaccination (OPV) campaign in Turkey, suggesting a causal relationship.Introduction Guillain-Barré syndrome (GBS) is a relatively rare disease (annual incidence: 1/100,000), usually presenting with symmetric progressive paralysis. The etiology of the disease is unknown.[1],[2] GBS has been frequently reported to be preceded by a non-specific infection of variable type, usually a few weeks before the onset of neurological symptoms.[3] Other suggested triggering factors include trauma, surgery or vaccination.[4] The last factor was frequently reported, especially during nationwide influenza or poliomyelitis vaccination campaigns.[5],[6] A nationwide campaign with live oral poliovirus vaccine (OPV) was organized to eradicate poliomyelitis in all parts of Turkey including our region, Eastern Turkey during May-June 2000. Five children with GBS were admitted to our hospital during or just after the campaign. In this article, we present the clinical and laboratory findings of these children. Our purpose is to emphasize that OPV may trigger GBS during a vaccination campaign. We wish to emphasize that oral polio vaccination during a campaign may trigger GBS in children, with neurological morbidity. Case Reports The study includes five children with GBS, younger than 5 years of age, admitted to the hospital between July 1 and August 31, 2000. The population of the Van province located in Eastern Turkey is approximately 300,000. The records of all patients with a diagnosis of GBS coded according to the International Statistical Classification of Diseases were evaluated. The clinical, laboratory and electrodiagnostic features described by Asbury and Cornblath in 1990 were used in the diagnosis of GBS.[7] Physical examination, routine urine and blood analyses, cerebrospinal fluid (CSF) examination, and electromyography (EMG) were performed. Virological studies on stool samples for determining the type of poliovirus were undertaken in all children. Clinical and laboratory findings of the patients are shown in [Table - 1]. By history, all children except Case 4 had received OPV before the onset of illness. OPV manufactured by Pasteur Merieux Connaught was received by all children. None of the patients who received OPV had a specific agent in stool cultures. CSF protein was found elevated in 3 patients (Cases 1, 2, 3), while CSF cell count was normal in all the cases. EMG was performed in 4 patients (Cases 1, 2, 4 and 5) and showed abnormalities typical of GBS (prolonged motor conduction velocity and absence of F-wave). EMG could not be performed in Case 3 because his general condition was poor and he died on the first day of admission. Virological examination of stool samples for poliovirus was found to be negative in all the children. Four patients were treated with intravenous immunoglobulin G (IVIG) (400 mg/kg/day for five days). Cases 1 and 3 (of whom one received IVIG) died of respiratory insufficiency. Discussion The role of vaccination in the cause of GBS is controversial. The risk in adults appeared to be high in 1976 after influenza immunization with the A/New Jersey/76 influenza vaccine, but no increase was noticed after influenza immunization in 1978 and 1979.[5],[8] An increased number of GBS cases both in children and in adults were observed during the OPV program.[9],[10] Kinnunen et al[6] examined 10 cases with onset of GBS within 10 weeks of OPV immunization during a nationwide OPV campaign. They reported that only 4 patients could recall recent symptomatic infection, and found no specific agent in these cases.[6] In the other study they noted that the results demonstrated a temporal association between poliovirus infection, caused by either wild type virus or live attenuated vaccine, and increased occurrence of GBS, but they could not prove the cause-effect relation between GBS and OPV administration.[1] Stratton et al[11] felt that the evidence favored acceptance of a causal relation between OPV and GBS. Contrary to previous studies, Ismail et al[12] found no correlation between OPV administration and GBS in 2 successive years (1995 and 1996) during a nationwide campaign targeting children less than 5 years of age. Rantala et al[2] also reported strong evidence against a causal relationship between OPV administration and GBS, by the failure to find a correlation between the usual age of immunization with OPV and the incidence of GBS by age, and the failure to find any children with the onset of GBS within 1 month of immunization with OPV. In our series all children were younger than 5 years of age. GBS was primarily related to OPV administration in all children except Case 4 in whom a history of viral gastroenteritis was present, which was well known as a triggering factor in the etiology of GBS.[13] When OPV was not given during 1999 we diagnosed only 2 children with GBS who were younger than 5 years of age in our clinic. Though the results are variable and the evidence is not robust, it is essential to consider OPV as a potential trigger for GBS in children, especially during a nationwide campaign and the children should be monitored. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=544;epage=545;aulast=Anlar The following images related to this document are available:Photo images[ni03174t1.jpg] |
| |||||||||

{kind=link}